The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2007;17(12)
Content
Lege Artis Medicinae
DECEMBER 20, 2007




Lege Artis Medicinae
DECEMBER 20, 2007

[MYELODYSPLASTIC SYNDROMES - NEW THERAPEUTIC OPTIONS]
[Myelodysplastic syndrome is a heterogeneous group of acquired clonal disorders of the haematopoietic stem cell characterized by ineffective haematopoiesis, peripheral cytopenia, and a high risk of progression to acute leukaemia. It is a common malignant disease with an increased incidence in the elderly population. Classification is based on a 1999 WHO recommendation, in which morphological features as well as clinical and cytogenetic characteristics are taken into account. Combined with the International Prognostic Scoring System (1997), it is suitable to predict prognosis and response to therapy. Clinical features include symptoms caused by anaemia, infections, and bleeding. Diagnosis is based on peripheral cytopenia and dysplastic morphology, as well as normal or increased cellularity in the bone marrow, with more than 10% of dysplastic cells. The verification of cytogenetic abnormalities is important both for confirming the diagnosis and predicting the prognosis. When designing the treatment strategy, it is essential to take the risk of leukaemia into account. On the other hand, the general state of the patient and the presence of accompanying diseases should also be considered. The goal of the treatment is to increase cell count and to decrease transfusion requirement, eventually to improve quality of life. Supportive therapy is an essential part of the management. In addition, growth factors, immunosuppressive and immunomodulatory agents, low-dose chemotherapy may be applied. Today, cure can only be achieved by allogenic stem cell transplantation. Recent findings in the epigenetic intracellular regulation allowed the definition of new therapeutic targets to develop drugs such as inhibitors of DNA methyltransferase and histone deacetylase.]
Lege Artis Medicinae
DECEMBER 20, 2007

[AUTOIMMUNE DISEASES TREATED BY AUTOLOGOUS HAEMOPOIETIC STEM CELLS]
[Autoimmune diseases are of multifactorial origin. Due to the disturbed immune tolerance, autoreactive T and B cells target self antigens, which lead to permanent organ damages. Despite of the recently introduced therapeutic protocols, the disease has a chronic course, in many cases with lethal outcome. The efficacy of stem cell therapy has been observed in animal models of autoimmune diseases and in autoimmune diseases associated with haematological disorders. Although this approach has been applied for more than 30 years, its widespread use has been delayed by the serious side effects caused by the conditioning treatments based on oncological protocols. The evaluation of the data of patients who had undergone autologous stem cell therapy revealed that the use of protocols for conditioning treatments that mostly cause lymphoablation, and also, if the procedures are carried out in specialized centres significantly reduce mortality, while the therapeutic efficacy remains optimal. Indications for autologous CD34+ stem cell therapy in patients with autoimmune diseases are internationally established and accepted. New, multicentric investigations have been launched in order to compare the efficacy of various protocols.]
Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

[PLEIOTROPIC FUNCTIONS OF ERYTHROPOIETIN]
[Erythropoietin produced by the foetal liver and the adult kidney is the major stimulator of erythropoiesis. Erythropoietin production is regulated by hypoxic activation of erythropoietin gene transcription. Recently, new sites of erythropoietin production have been found mainly in the central nervous system and in the cardiovascular system. These tissues have a paracrine and/or autocrine system of erythopoietin. The pleiotropic function of erythropoietin in these systems is tissue and cell protection by several mechanisms including inhibition of apoptosis, attenuation of ischaemic or reperfusion injury, anti-inflammatory and antioxidative effects. Furthermore, it promotes vascular recovery and enhances neoangiogenesis. In vivo and in vitro studies have proved that systemically administered human erythropoietin can also provide tissue protection. However, adverse effects of erythropoietin treatment such as hypertension, hyperviscosity and thrombosis may override the beneficial effect of systemic erythropoietin treatment. There are preliminary data that erythropoietin analogues, e.g., asyaloerythropoietin or carbamylated erythropoietin can provide tissue protection without stimulating erythropoiesis.]
Lege Artis Medicinae
DECEMBER 20, 2007

[THE ROLE AND METHODS OF IMPROVING INSULIN SENSITIVITY AND BETA-CELL FUNCTION IN TYPE 2 DIABETES]
[Increased knowledge on the pathogenesis of type 2 diabetes has considerably transformed the principles and practice of treatment. Insulin resistance and beta-cell dysfunction, the two main components of the pathogenesis both play a role in the conversion of normal glucose metabolism, through impaired glucose tolerance, into type 2 diabetes. Decreased insulin sensitivity, with or without beta-cell dysfunction, is present in the vast majority cases, therefore, its treatment is essential. Physical activity is known to improve insulin sensitivity. The primary action of the recommended first-line pharmacological agent metformin is the inhibition of hepatic glucose production but it also moderately stimulates muscle glucose uptake. Glitazones are insulin sensitizers that increase glucose uptake in muscle and adipose tissue and moderately decrease hepatic glucose production. Some evidence suggests that α-glucosidase inhibitors and also certain insulin secretagogues can improve the effect of insulin. Early detection of the pathologic state and an efficient treatment to improve both insulin sensitivity and beta-cell function are essential in order to slow the progression and prevent the development of complications in type 2 diabetes.]
Lege Artis Medicinae
DECEMBER 20, 2007
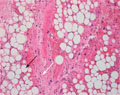
[RETROPERITONEAL LIPOSARCOMA]
[INTRODUCTION - Liposarcoma is a malignant soft tissue tumour, which represents less than 0.1% of all human cancers. Approximately 20% of liposarcomas arise in the retroperitoneum. Radical surgical excision is potentially curative, making it the first choice of treatment. For local tumour control palliative chemo- and/or radiotherapy can be used. CASE REPORT - A 28-year-old man with a history of weight loss, fatigue and abdominal tightness was diagnosed to have a giant dedifferentiated retroperitoneal liposarcoma, which showed aggressive growth and gave local recurrences. Multiple surgical excisions were performed, the first two times with curative, subsequently with palliative intent. To reduce the retroperitoneal tumour mass, several chemotherapeutic regimens were applied with complementary radiotherapy. As a result of the combinational therapy, tumour growth stopped temporarily, pressure pain subsided and the patient's quality of life was satisfactory. Finally, distant metastases developed in the bones of the right hip, in the lung and on the serous membranes and after 44 months of follow-up the patient died. CONCLUSION - It has been postulated that ifosfamide and doxorubicin based combined chemotherapy prevents or postpones the development of distant metastases. Considering the significant risk of local and distant recurrences, the use of ifosfamide-doxorubicin based combined chemotherapy is recommended in highgrade retroperitoneal liposarcoma, even following complete surgical excision.]
Lege Artis Medicinae
DECEMBER 20, 2007

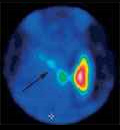
[A CASE OF MISIDENTIFIED SYNCHRONOUS COLON CANCER]
[INTRODUCTION - Synchronous colorectal cancers are not uncommon, therefore, total colonoscopy is indicated even in cases of distally located large bowel carcinomas. CASE REPORT - An 84-year-old man had emergency surgery because of bowel obstruction and a node-negative carcinoma of the sigmoid colon was removed according to Hartmann. Before the reconstruction of bowel continuity, colonoscopy revealed a relatively small polypoid tumour in the right colon, unsuitable for colonoscopic polypectomy. Two localization clips were then inserted at the site of the endoscopic biopsy that later resulted in the diagnosis of adenocarcinoma. At the time of the reconstruction surgery, an appendectomy was also performed and, though the clips were not found, the polypoid tumour was removed through appendectomic orifice. The polyp thus removed, however, proved to be an adenoma. A repeated colonoscopy and biopsy confirmed both the localization clips and the malignant nature of the remaining right-sided lesion, which was finally removed with right hemicolectomy. CONCLUSION - Anatomic localization of rightsided colon cancers by colonoscopy is often imprecise. The correct identification of a malignant tumour may be compromised by a nearby benign lesion. If a lesion was labelled by some means, the localization sign should be identified both intraoperatively and during the gross pathologic work-up, asking for external help (e.g., radiology in case of a metal clip) if necessary.]
Lege Artis Medicinae
DECEMBER 20, 2007
Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007
Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

Lege Artis Medicinae
DECEMBER 20, 2007

1.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
2023 27. NOV
2.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
2023 27. SEP
3.
Clinical Neuroscience
Neuropathic pain and mood disorders in earthquake survivors with peripheral nerve injuries
2024 03. APR
4.
Journal of Nursing Theory and Practice
[Correlations of Sarcopenia, Frailty, Falls and Social Isolation – A Literature Review in the Light of Swedish Statistics]
2023 31. OCT
5.
Clinical Neuroscience
[Comparison of pain intensity measurements among patients with low-back pain]
2024 03. APR
1.
Clinical Neuroscience Proceedings
[A Magyar Stroke Társaság XVIII. Kongresszusa és a Magyar Neuroszonológiai Társaság XV. Konferenciája. Absztraktfüzet]
2024 06. SEP
2.
3.
Journal of Nursing Theory and Practice
[A selection of the entries submitted to the literary contest "Honorable mission: the joys and challenges of our profession" ]
2024 02. SEP
4.
Journal of Nursing Theory and Practice
[End of Life and Palliative Care of Newborns in the Nursing Context]
2024 02. SEP
5.
Journal of Nursing Theory and Practice
[Aspects of Occupational Health Nursing for Incurable Patients ]
2024 02. SEP