The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2022;32(10)
Content
Lege Artis Medicinae
OCTOBER 28, 2022

[Dear Reader!]
[2022 őszén a LAM ismét megújult, ennek a folyamatnak a részeként tematikus lapszámmal jelentkezünk. Ennek 2022 októberében több apropója is van: egyrészt a Semmelweis Egyetem Családorvosi Tanszéke prof. Torzsa Péter (lapunk szerkesztőségi tagjának) szervezésében ez év májusában hypertonia témájú rezidensképzést szervezett, igen nagy sikerrel. Torzsa professzor úr felkérésére a rezidensképzés előadói megírták előadásaikat, és a LAM büszke arra, hogy ezeket közreadhatja. ]



Lege Artis Medicinae
OCTOBER 28, 2022

[The epidemiology, classification of hypertension and the Importance of risk stratification]
[Hypertension, which is the most important independent risk factor of cardiovascular mortality, affects approximately 3.5 million people in Hungary. Among them the rate of the unknown, known, but untreated or uncontrolled hypertensive patients is more, than 50%, a fact, which underlines the importance of screening and proper treatment. Since 2017, there is a difference in the classification of hypertension between Europe and the United States, based mostly on SPRINT study, which was published in 2015. However, in the treatment recommendations more similarities are present. Risk stratification must be the part of hypertension care. In risk communication as an alternative, the concept of vascular age was introduced, which mirrors more suggestively the patients' vascular hazard. In this review the author overviews the novelties in hypertension epidemiology, classification, and risk stratification.]
Lege Artis Medicinae
OCTOBER 28, 2022

[Measurement of blood pressure. White-coat and masked hypertension]
[The diagnosis of hypertension is important, as high blood pressure is the most frequent and consequently the most important risk factor of cardiovascular diseases leading to mortality. The basis of diagnosis is the correct blood pressure measurement. Recent guidelines underline the importance of out of office (home and ambulatory) blood pressure monitoring besides the traditional office measurements. These methods have not only additive prognostic value, but with the help of these measurements, special hypertension forms (white coat and masked hypertension) can be diagnosed. On top of all these, home monitoring increases the patient’s compliance to the therapy. This short review summarizes the most important information on blood pressure measurement.]

Lege Artis Medicinae
OCTOBER 28, 2022

[Target blood pressure range and non-pharmacologic treatment of high blood pressure ]
[International guidelines, thus the Hungarian guidelines too, recommend the use of the target blood pressure range instead of target blood pressure values since it is more in line with needs of the everyday practice. While caring for high blood pressure patients, to start non-pharmacological treatment (lifestyle changes, reducing excess weight, smoking cessation, reducing salt consumption, and the regular physical activity) as soon as possible is of pre-eminent importance. Physical activity is recommended at least 3-4 times a week, for 30 to 60 minutes. In case of borderline hypertension, physical activity results in an average blood pressure reduction of 6/7 mmHg. It is recommended to achieve and maintain a normal body mass index (BMI between 20 and 25), to consume less than 5 g of sodium chloride a day, to eat more fruits and vegetables, and dairy products and foods of low trans fat content. It is advisable to reduce alcohol consumption to less than 20-30 g/day of ethanol for men and less than 10-20 g/day of ethanol for women. Quitting advice should be given to tobacco smoking patients.]
Lege Artis Medicinae
OCTOBER 28, 2022

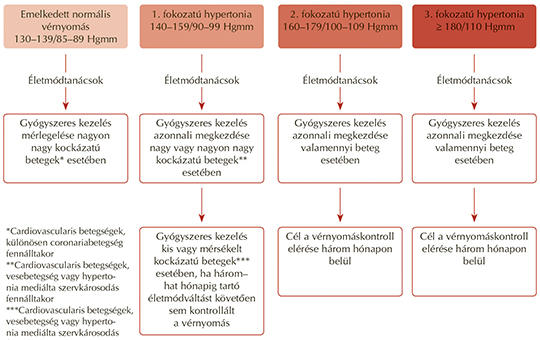
[Drug treatment strategies, hypertensive urgencies and emergencies]
[In this paper I summarise the currently valid guidelines for the pharmacotherapy of hypertensive patients, and in separate part, those for hypertensive urgencies and emergencies.]
Lege Artis Medicinae
OCTOBER 28, 2022

[Resistant and secondary forms of hypertension]
[Hypertension is the leading risk factor for cardiovascular events and mortality worldwide. In the case of resistant hypertension, the risk of hypertension-related cardiovascular and renal morbidity and mortality is increased despite the therapy. The prevalence of secondary hypertension is extremely high in patients with true resistant hypertension. Without an adequate treatment in time severe complications may occur frequently, therefore screening is mandatory in every case. Among more important secondary hypertensions, the clinical recommendations for diagnosis and therapy of obstructive sleep apnea, primary aldosteronism, renovascular hypertension and phaeochromocytoma/paraganglioma are discussed.]
Lege Artis Medicinae
OCTOBER 28, 2022

[Novelties in childhood hypertension ]
[Childhood hypertension was previously regarded as a rare disease, caused primarily by renal or renovascular diseases. However, in the past 10-15 years due to increased prevalence of childhood obesity and the associated metabolic abnormalities, elevated blood pressure has become significantly more common. This highlights the public health significance of high blood pressure, and it also determines the screening protocols, which varies by age groups. The child's development should be taken into account when establishing normal blood pressure in childhood. In addition to the definition of hypertension, the characteristics of blood pressure measurements must also be known. Before adolescence, hypertension is most likely caused by an organic cause. During puberty and postpuberty, hypertension is primarily associated with obesity. The tests and their evaluation should be performed in a centre familiar with the examination of children, and where the childhood normal values are known. The goal of therapy is to prevent the organ-damaging effects of hypertension in a population where the disease is expected to persist for decades. Customized and realistic lifestyle changes are essential during treatment, but it may be necessary to introduce drug therapy as well. The medication should start as a monotherapy with the lowest necessary dose. If this does not achieve an adequate therapeutic effect, the treatment is supplemented with another class of antihypertensive medication.]
Lege Artis Medicinae
OCTOBER 28, 2022
[How and what can we do together for the care of hypertensive patients in communities of practice?]
[As the first step in the transformation of primary care, the first communities of practice were set up to seek ways of expanding the competences, the range of equipment and the services provided by primary care. The structure of these no longer resembles the previous model of general practice, with teams of two or three doctors working in isolation from each other. The new form is a network of community practices. The care and management of hypertensive patients is a typical area of community work. In this article, the authors aim to illustrate the role of community practices in the care and management of hypertensive patients.]
Lege Artis Medicinae
OCTOBER 28, 2022

Lege Artis Medicinae
OCTOBER 28, 2022

[Clinical implication of assessment of vascular age]
[Arterial aging is a physiologic process coexisting with general aging of the human body, however arterial age of a given individual can be different from his chronologic age. The underlying causes are determined by genetic factors, cell biologic processes and several risk factors. While risk scores are invaluable tools for adapted preventive strategies, a significant gap exists between predicted and actual event rates. Therefore, it is necessary to refine the risk stratification at an individual level, the tools for this are biomarkers. Biomarkers are surrogate endpoints, which precede, substitute the real, hard endpoint clinical events. It has been proposed that numerous potential vascular biomarkers would have a role in primary and secondary cardiovascular prevention. Most of them fit in the concept of early vascular aging (EVA). Only carotid ultrasonography, ankle-brachial index and carotid-femoral pulse wave velocity meet perfectly the strictest criteria against the biomarkers. The process of arterial aging may be decelerated and beneficially influenced with non-pharmacologic and pharmacologic treatment strategies.]
Lege Artis Medicinae
OCTOBER 28, 2022

[The role of the Janus-faced ACE2-protein and its practical importance]
[The renin-angiotensin-aldosteron system is of pivotal importance in maintaining the homeostasis of human organism, however its pathological overactivity plays a significant role in the development of hypertension, hypertensive organ damages and heart failure. While maintaining and regulating the proper balance of the RAAS, one of the carboxipeptidase enzymes, namely the ACE2-protein has a crucial role. In addition, the cell membrane-linked ACE2 functions also as a receptor of the SARS-CoV 2 virus allowing it to penetrate the cells and develop COVID-19 disease, which caused the worldwide pandemic in recent years. Based on these facts, ACE2 may be named properly as a “Janus-faced” protein. Using pharmaceutically its beneficial role in regulating RAAS activity, angiotensin receptor blockers e.g. olmesartan can provide effective blood pressure lowering and cardiovascular protection.]
Lege Artis Medicinae
OCTOBER 28, 2022

Lege Artis Medicinae
OCTOBER 28, 2022
Lege Artis Medicinae
OCTOBER 28, 2022

1.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
2023 27. NOV
2.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
2023 27. SEP
3.
Clinical Neuroscience
Neuropathic pain and mood disorders in earthquake survivors with peripheral nerve injuries
2024 03. APR
4.
Journal of Nursing Theory and Practice
[Correlations of Sarcopenia, Frailty, Falls and Social Isolation – A Literature Review in the Light of Swedish Statistics]
2023 31. OCT
5.
Clinical Neuroscience
[Comparison of pain intensity measurements among patients with low-back pain]
2024 03. APR
1.
Clinical Neuroscience Proceedings
[A Magyar Stroke Társaság XVIII. Kongresszusa és a Magyar Neuroszonológiai Társaság XV. Konferenciája. Absztraktfüzet]
2024 06. SEP
2.
3.
Journal of Nursing Theory and Practice
[A selection of the entries submitted to the literary contest "Honorable mission: the joys and challenges of our profession" ]
2024 02. SEP
4.
Journal of Nursing Theory and Practice
[End of Life and Palliative Care of Newborns in the Nursing Context]
2024 02. SEP
5.
Journal of Nursing Theory and Practice
[Aspects of Occupational Health Nursing for Incurable Patients ]
2024 02. SEP