The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2021;31(07)
Content
Lege Artis Medicinae
JULY 13, 2021



Lege Artis Medicinae
JULY 13, 2021
[Mechanism of mucosal defence and options to reduce virus invasion during the COVID pandemic]
[The portal of entry for coronavirus is the mucous membrane of the respiratory tract. Severity, organ manifestations and outcome of COVID-19 are determined by the viral load, burdening the attacked organism. Condition of the respiratory tract and gastrointestinal mucosa and the capacity of their defence system are crucial for virus penetration, fusion with epithelial cells and replication. Direct neural spread, penetration into the deeper airways and spread through the lymph nodes depend on these functions. Virus binding and engulfment is an active process. The virus penetrates the endosomes of the epithelial cell, by enzymatic transfer where it is recognised by natural defence agents and triggers the first defence responses. These alarm the entire immune system and trigger a whole chain of inflammatory and enzymatic defence processes (cytokine and bradykinin storm) proportional to the viral load. The severity endpoint of COVID-19 pathology is alveolitis, cerebral vasculitis and intestinal damage, often with fatal outcome. The airway mucosa defends itself by secreting surface factors and recruiting and activating cells of the adaptive immune system. An important element of the latter is the early appearance of secretory IgA in the mucosa. The viral invasion can be prevented by application of a nasal spray containing carrageenan, which engages the virus and prevents its attachment by the gel-forming property of carrageenan. This effect has worked in previous virus epidemics and the first COVID-19 experiences confirm its protective role. ]
Lege Artis Medicinae
JULY 13, 2021

[Neurological complications of COVID-19]
[The SARS-CoV-2 virus of COVID-19 is present in all countries of the world by 2021 causing primarily respiratory symptoms by penumonia with severe respiratory failure. Since the early stages of the pandemic, there were published case reports and comprehensive clinical studies about the neurological symptoms and complications of the infection (e.g. myalgia, anosmia, ageusia, encephalitis, encephalopathy, cerebrovascular conditions, Guillain-Barré syndrome and specific neuropathies). As it is well known, drugs used in therapeutic research may also have neurological adverse effects. Our summary aims to provide a practical overview of domestic and international literature about the already known neurological complications of SARS-CoV-2 infection.]
Lege Artis Medicinae
JULY 13, 2021
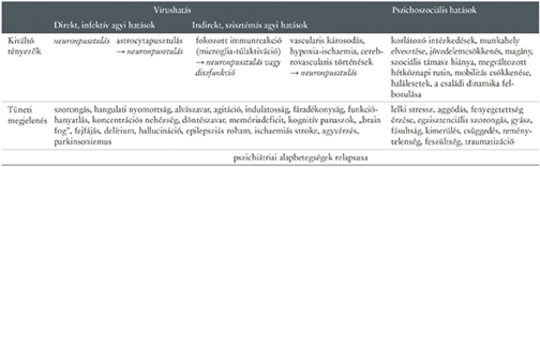
[Neuropsychiatric complications of COVID-19 infection]
[Initially, the studies of COVID-19 infection focused primarily on the acute and subacute somatic symptoms of limited duration, but later on with the spread of the pandemic the scope was extended to prolonged symptoms recognized as complications. Data are mounting about after-effects in circulation, respiration, coagulation, problematic outcomes in rheumatology, dermatology, ophthalmology, as well as about the acute and prolonged symptoms of the dysfunctional central nervous system. Initially, sporadic case reports, later results of population based studies and animal models were available, and the first systematic review articles were emerging during preparation of our survey. Lesions of the central nervous system may manifest themselves both in neurological symptoms and diseases or psychiatric complaints and syndromes. The scale of symptoms is broad, the pathomechanisms are not perfectly mapped thus all therapeutic approaches are in their infancy yet. Epidemiological data of neuropsychiatric complications are incomplete for the time being though they have been rapidly becoming more accurate. Conservative estimates assume tens of millions of people affected worldwide. More time is necessary to assess the persistence or improvement of the prolonged symptoms. Besides every efforts to block the spread of the virus, the utmost importance is to analyze the effects of the virus on the central nervous system and to develop effective treatment strategies. According to our current knowledge, the pathomechanism of neuropsychiatric complications is multifactorial. Beyond the direct deleterious effect of the virus on neuronal and glial functions, more important is that the serious consequences of cerebrovascular dysfunction and poor oxygenation have to be taken into consideration together with extended and prolonged systemic immunological processes, which markedly harm the brain tissue, notably neurons, axons, synapses and glia cells. Based on a non-systematic literature review our work details these mechanisms and addresses therapeutic options as well. ]
Lege Artis Medicinae
JULY 13, 2021

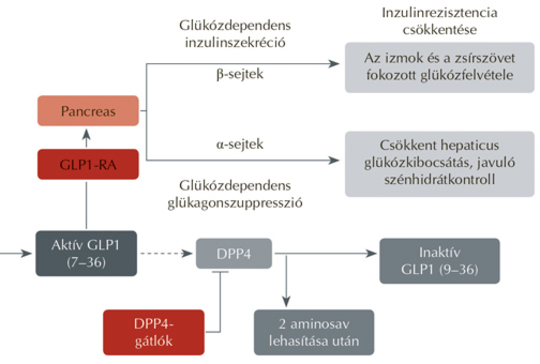
[Potential benefits of using GLP1-receptor agonists during COVID-19 epidemic]
[The risk of SARS-CoV-2 infection is higher among diabetic patients. The severity of progressing infection also increases in diabetes mellitus. Obesity associated with diabetes and cardiovascular disease are worsening the prognosis. Glucagon-like peptide-1 receptor agonists (GLP1-RA) administered in type 2 diabetes are lowering significantly the blood sugar level without increasing the risk of hypoglycaemia, support patients to lose weight, and reduce the likelihood of developing and worsening cardiovascular diseases. Through their many effects, they prepare diabetic patients to a certain extent to survive SARS-CoV-2 infection with fewer complications and have a beneficial immunological effect against the development of cytokine storm respectively. The authors summarize the potential beneficial effects of GLP1-RAs in SARS-CoV-2 infection.]
Lege Artis Medicinae
JULY 13, 2021

[Face mask associated dry eye syndrome during the COVID-19 pandemic]
[During the COVID-19 pandemic, the use of face mask was mandated to slow down also this way the spread of SARS-CoV-2. Dry eye syndrome is a multifactorial, common disease of the tear film and ocular surface, which has a significant negative effect on quality of life. The face mask and prolonged use of digital devices in home office and on-line school education raised the prevalence of dry eye syndrome among the patients. Eye irritation caused by the use of masks increased the risk of infection through the eye surface. This study concerns the effect of mask use on the eye surface during the COVID-19 pandemic, the prevention of this condition and its therapy options respectively.]
Lege Artis Medicinae
JULY 13, 2021
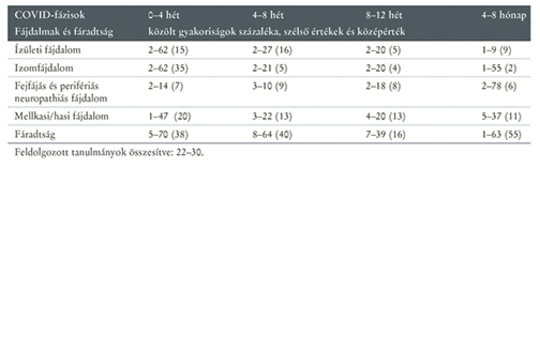
[Treatment options for localized and widespread post-COVID pain]
[Data on the new coronavirus caused disease and its treatment have been accumulating for more than a year. There are four main disease courses: no or mild symptoms, unavoidable hospitalisation, severe or lethal outcome, and permanent or post-hoc manifestations. The last course is usually referred to as post-COVID syndrome. As a part of the acute and post-COVID symptomatology there were published pain perceptions with frequent but heterogeneous localisation. It is practical to classify them by the origin of pain: nociceptive/inflammatory, peripheral neuropathic or central. Additionally, we have to clear which phase is the post-COVID patient in i.e. the patient has the prolonged COVID- or persistent post-COVID syndrome. However, in addition to an acute general inflammatory reaction, a true inflammation of joints and muscles is very rare in the musculoskeletal system. The diffuse musculoskeletal pain, chronic fatigue, generalised anxiety and depressive disposition manifest themselves in both acute and persistent forms. Their explanation is essentially of neurological nature: there are para-infectious “neuro-inflammation”, i.e. neuropathic and central mechanisms in the background. Accordingly, therapeutic options must be chosen while concerning the neuropharmacological action mechanisms of analgesics. Elderly patients at high iatrogenic risk and with multiple co-morbidities may be treated transdermal instead of oral drug administration.]
Lege Artis Medicinae
JULY 13, 2021

Lege Artis Medicinae
JULY 13, 2021

Lege Artis Medicinae
JULY 13, 2021
Lege Artis Medicinae
JULY 13, 2021

[COVID-19 skin symptoms]
[We observed many coronavirus associated skin symptoms during the 3rd wave of the COVID-19 (Sars-CoV-2) pandemic in Hungary. The skin lesions include viral exanthems, urticariform rash, vesicles of different size, pernio-like lesions, vasculopathic phenomena of various stages of severity or skin symptoms like pityriasis rosea or erythema multiforme as well as rash resembling Kawasaki’s disease. Some of these indicate the presence of primary skin infection caused by the COVID-19 viral infection others may be lesions accompanying respiratory tract infection or may be manifestations of the patient’s immune response. The focus of the present study has been the most prevalent skin symptoms including the mildest to the most severe forms. Numerous hypotheses have been come up regarding the origin of these skin lesions but no clear explanations have been published in the relevant evidence-based medical literature. Diagnosing skin manifestations associated with COVID-19 infection may be helpful to identify infected patients, start appropriate therapy and implement preventive public health measures in a timely fashion.]
Lege Artis Medicinae
JULY 13, 2021

Lege Artis Medicinae
JULY 13, 2021

1.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
2023 27. NOV
2.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
2023 27. SEP
3.
Clinical Neuroscience
Neuropathic pain and mood disorders in earthquake survivors with peripheral nerve injuries
2024 03. APR
4.
Journal of Nursing Theory and Practice
[Correlations of Sarcopenia, Frailty, Falls and Social Isolation – A Literature Review in the Light of Swedish Statistics]
2023 31. OCT
5.
Clinical Neuroscience
[Comparison of pain intensity measurements among patients with low-back pain]
2024 03. APR
1.
Clinical Neuroscience Proceedings
[A Magyar Stroke Társaság XVIII. Kongresszusa és a Magyar Neuroszonológiai Társaság XV. Konferenciája. Absztraktfüzet]
2024 06. SEP
2.
3.
Journal of Nursing Theory and Practice
[A selection of the entries submitted to the literary contest "Honorable mission: the joys and challenges of our profession" ]
2024 02. SEP
4.
Journal of Nursing Theory and Practice
[End of Life and Palliative Care of Newborns in the Nursing Context]
2024 02. SEP
5.
Journal of Nursing Theory and Practice
[Aspects of Occupational Health Nursing for Incurable Patients ]
2024 02. SEP