The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2020;30(03)
Content
Lege Artis Medicinae
MARCH 10, 2020




Lege Artis Medicinae
MARCH 10, 2020

[Summary data of Hungary's comprehensive health screening program (MAESZ) 2010-2019]
[The comprehensive screening program of Hungary (MAESZ) 2010-2020-2030 is a unique initiative in Hungary and worldwide too. This largest humanitarian program provides by the latest technology free screening tests for all residents in Hungary. The program developed by 76 professional organizations offers 38 screening tests to every participants free of charge, in a special designed screening truck. Screening program performed by MAESZ includes cardiovascular, ophthalmologic, dermatologic, gynecologic, and neurologic investigations, lab tests, audiometry, blood pressure and arterial stiffness measurements, and venous Doppler ultrasound examinations. Moreover, screening tests for lactose intolerance, colon malignancy, inflammatory bowel disease, reflux disease, urine incontinency, prostatic cancer and physical activity level were evaluated. Starting 2020, a dental screening station will be added to the mobile unit for early detection of oral cancers. Beyond screening tests, special attention is paid to assess health threatening risk factors, such as smoking, alcohol consumption, physical inactivity, unhealthy nutrition, and obesity. The program demonstrates the key elements of first aid from reanimation to bandage of burns in cooperation with professional and civil organisations. Furthermore, during the waiting time, participants get lifestyle recommendations and a health booklet with a bar code enabling the immediate computer analysis of test outcomes. Since the 2018/2019 school year the official prevention program for children entitled “Travel around the Empire of Health” was started. During its 10 years, the MAESZ performed 7 million free of charge screening tests on 1,886 scenes, enrolled 560,000 participants, invested 16,000 hours for prevention, handed out 1,200,000 health booklets and 391,000 prevention info packages to thousands of families. More than 20,000 health professionals (GPs, nurses, dietetics, health development agents, public health government officials, Accident Prevention Committee of National Police Headquarters, General Directorate of Social Affairs and Child Protection and non-governmental organizations) have been participated. The program designed to improve social health aims to help more and more Hungarian citizens to be informed about their health status and to reminds them of the importance of prevention. ]
Lege Artis Medicinae
MARCH 10, 2020

[Recommendations of the European Atherosclerosis Society (EAS) and the European Society of Cardiology (ESC) for dyslipidaemia. Focused on: primary prevention]
[In 2019 the European Atherosclerosis Society (EAS) and European Society of Cardiology (ESC) renewed their dyslipidaemia guidelines. The new version is more progressive than the previous ones. Thus, in the low-risk, not severely hypercholesterolaemic population cholesterol-lowering medication is also suggested. Except this low-risk group, atherogenic target values, e.g. for LDL-cholesterol, were reduced by an entire category, in some cases to the lowest one. If these goals cannot be achieved with statin-monotherapy, combined treatment is recommended generally by the cholesterol inhibitor ezetimib, and in some very high-risk cases also by innovative cholesterol lowering so-called PCSK9 inhibitor. ]
Lege Artis Medicinae
MARCH 10, 2020

Lege Artis Medicinae
MARCH 10, 2020

[Primary care strategy of antihypertensive treatment of very elderly and frail patients]
[BACKGROUND - When treating very elderly and frail hypertensive patients, there have to be taken in account the general health condition and frailty of patients, the present cardiovascular diseases (CVD) and values of the systolic blood pressure (SBP). Goals - In a clinical study performed in 29 countries, we aimed to analyse differences in practical antihypertensive therapy of family doctors among patients older than 80 years; further we sought to answer how much was influenced their therapeutic choice by frailty of the old age. The other goal of our study was to compare Hungarian versus international outcomes. Methodology - As part of an online survey, family practitioners had to decide about necessity of starting antihypertensive treatment among very elderly patients according to different patterns of frailty, SBP and CVD. The ratio of specific cases with positive treatment decision of family practitioners was compared in all 29 countries. We used a logistic mixed model analysis to multivariately model the role of frailty. Results - 2543 family practitioners participated in the cross-national study; 52% were female; 51% practised in urban environment. In 61% of practices, there was the ratio higher than 10% of very elderly patients. Hungary participated with 247 family practitioners in the study; 52.3% were female; 63.1% practised in urban environment. In 48.8% of practices the ratio of very elderly patients was higher than 10%. In 24 out of the 29 countries (83%), frailty was associated with GPs’ negative decision about starting treatment even after adjustment for SBP, CVD, and GP characteristics (odds ratio [OR 0.53]), 95% CI: 0.48-0.59; ORs per country 0.11-1.78). The lowest treatment ratio was in the Netherlands (34.2%; 95% CI: 32.0-36.5%) and the highest one in Ukraine (88.3%; 95% CI: 85.3-90.9%). In Hungary’s treatment ratio ranged 50-59%. This country ranked on the 27th place since Hungarian family practitioners chose rather to start antihypertensive treatment despite the frailty of the patient (OR=1.16; 95% CI: 0.85-1.59). Hungarian family practitioners started pharmacotherapy of elderly patients more frequently if they were males (OR= 1.45; 95% CI: 0.81-2.61), were working in their practice for less than 5 years (OR=2.41; 94% CI: 0.51-11.38), and if they had many patients aged over 80 years in their practice (OR=2.18; 95% CI: 0.70-6.80), however these differences were statistically not significant. Among Hungarian family practitioners starting therapy was significantly influenced by cardiovascular disease (OR=3.71; 95% CI: 2.64-5.23) and a SBP over 160 mmHg (OR=190.39; 95% CI: 106.83-339.28). Conclusions - In our study, there was significant difference between countries in starting antihypertensive treatment for very elderly patients. However, Hungary was among the countries where family practitioners preferred to treat their frail patients. The patients’ frailty did not have any impact on starting the therapy; rather cardiovascular disease and a SBP over 160 mmHg decided. It is an important message of the study that there is continuous need to educate family practitioners and trainees about the treatment of frail, elderly hypertensive patients.]
Lege Artis Medicinae
MARCH 10, 2020

[Nutritional status, realizing sarcopenia and the importance of prehabilitation in surgical departments]
[INTRODUCTION - Malnutrition can significantly influence the surgery’s outcomes. Currently, patients risk grouping is based on the body mass index (BMI), and the preparation for surgery is concerned only as nutrients administration. PATIENTS AND METHODS - The Nutrition Support Team established in our Department is assessing first the patients’ nutritional status (BMI, MUST), sarcopenia (skinfold measure, handgrip strength) and fitness status (6 min step test, sit to stand test). Risk group patients were suggested nutrients and physiotherapy prior to the surgical operation. In order to follow up our patients we created an online interface and repeated the tests immediately before the operation. RESULTS - 135 cancer patients (76 male and 59 female) were operated. Their average age was 69.6 years. 33 patients had weight loss before the first consultation (average=8.7 kg). Their average BMI was 26.3. 21 patients had gained weight in the last 6 months (average=7.8 kg). Patients with left descending colon, liver - and also pancreatic tumors had overweight BMI values while the rest of patients ill with right colon and stomach neoplasm had normal weight. Those patients who we enrolled to the online system had better results at the second assessment. CONCLUSIONS - According to our survey, most of the patients had overweight BMI values but had sarcopenia based on anthropometric tests. Therefore, the importance of in time recognized and preoperatively started nutritional therapy must be coupled with the parallel applied physiotherapy. ]
Lege Artis Medicinae
MARCH 10, 2020

[Diagnosis and treatment of the overactive bladder]
[The Overactive Bladder Syndrome (OAB) is a symptomatic diagnosis featured mainly by urgency of urine discharging. This condition can be triggered by a number of etiological factors, most of which are idiopathic in origin. Regardless of gender and age, the prevalence is ca. 16% and has a serious impact on the quality of life of the patients. Investigations are mostly performed through usual baseline examinations; second-line invasive examinations are rarely required. The broad spectrum of treatment options ranges from lifestyle changes and elimination of triggering factors, through behavioural therapy and medication to the minimally invasive (botulinum toxin, neuromodulation, percutaneous stimulation of the tibial nerve) - and rarely - invasive therapies. ]
Lege Artis Medicinae
MARCH 10, 2020
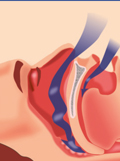
[The role of dyslipidaemia in the patomechanism of obstructive sleep apnoea ]
[Obstructive sleep apnoea (OSA) is the most recent sleep-breathing disorder, which is characterised by repetitive collapses of the upper airways. Chronic intermittent hypoxia, sleep fragmentation and systemic inflammation play pre-eminent role in the pathogenesis of OSA and its comorbidities, such as dyslipidaemia. The triple impaired lipid metabolism results in OSA by dysregulated lipid synthesis of the liver, insufficient lipoprotein clearance and increased lypolysis. Several previous studies examined the association between dyslipidaemia and OSA with various outcomes. The aim of this review is to present the pathomechanism of dyslipidemia in the OSA. ]
Lege Artis Medicinae
MARCH 10, 2020

Lege Artis Medicinae
MARCH 10, 2020

Lege Artis Medicinae
MARCH 10, 2020

Lege Artis Medicinae
MARCH 10, 2020

1.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
2023 27. NOV
2.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
2023 27. SEP
3.
Clinical Neuroscience
Neuropathic pain and mood disorders in earthquake survivors with peripheral nerve injuries
2024 03. APR
4.
Journal of Nursing Theory and Practice
[Correlations of Sarcopenia, Frailty, Falls and Social Isolation – A Literature Review in the Light of Swedish Statistics]
2023 31. OCT
5.
Clinical Neuroscience
[Comparison of pain intensity measurements among patients with low-back pain]
2024 03. APR
1.
Clinical Neuroscience Proceedings
[A Magyar Stroke Társaság XVIII. Kongresszusa és a Magyar Neuroszonológiai Társaság XV. Konferenciája. Absztraktfüzet]
2024 06. SEP
2.
3.
Journal of Nursing Theory and Practice
[A selection of the entries submitted to the literary contest "Honorable mission: the joys and challenges of our profession" ]
2024 02. SEP
4.
Journal of Nursing Theory and Practice
[End of Life and Palliative Care of Newborns in the Nursing Context]
2024 02. SEP
5.
Journal of Nursing Theory and Practice
[Aspects of Occupational Health Nursing for Incurable Patients ]
2024 02. SEP