The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2004;14(02)
Content
Lege Artis Medicinae
FEBRUARY 21, 2004




Lege Artis Medicinae
FEBRUARY 21, 2004

[POSTMENOPAUSAL HYPERTENSION]
[Women with normal cycles on the average have lower blood pressure than age matched men. From the fifth decade of life increasing average blood pressure values of females reach or even exceed the levels of males. The frequency of hypertension among women in menopause and postmenopause is 3-4 times greater than in premenopause. This great difference can not be explained by the age dependent increase in blood pressure. There are several pathological components in the background of the elevation of blood pressure following the reduction and failure of female sex hormone production. Among these components are lifestyle changes, reduced physical activity, growing body weight, increased sympathetic activity, higher RAS (renin-angiotensin system) influence and increased salt dependence of blood pressure seem to be the dominant factors. Contrary to earlier suggestions recent clinical findings have proved that estrogen or combined hormone replacement therapy did not increase but rather slightly reduced the blood pressure in menopausal and postmenopausal hypertensive women. Therefore, hypertension itself should not be the contraindication against carefully managed hormone replacement therapy. The therapy is frequently used for preventing severe osteoporosis in spite of the disappointing cardiovascular results of the WHI and HERS trials. In the Joint National Committee 7 there are no special recommendations which would strictly prefer one or another antihypertensive agents in the pharmacological treatment of postmenopausal hypertension. However doctors are assisted in their individual therapeutical decisions by certain clinical and experimental findings which refer to higher sympathic activity, enhanced RAS influence and increased salt dependency in the pathomechanism of postmenopausal hypertension.]
Lege Artis Medicinae
FEBRUARY 21, 2004

Lege Artis Medicinae
FEBRUARY 21, 2004

Lege Artis Medicinae
FEBRUARY 21, 2004

[THE HISTORY OF FLUOROQUINOLONES]
[During the 40 year history of quinolones, from the first compounds (nalidixic acid, oxolinic acid, norfloxacin) suitable only for the treatment of mild urinary tract infections, an important group of antimicrobials was developed that can be used for the treatment of serious Gramnegative (ciprofloxacin, ofloxacin) and Grampositive (levofloxacin, moxifloxacin) infections. With the changes in the antimicrobial spectrum of the new derivatives it seems, that the clinical indications of the mainly anti-Gram-positive and the mainly anti-Gram-negative fluoroquinolones can be separated. We also learned the characteristics of their antibacterial activity that makes the optimal administration possible assuring the maximum clinical efficacy and the minimal development of bacterial resistance. The activity of fluoroquinolones can also be compromised by bacterial resistance so to preserve their clinical value it is important to follow the above mentioned principles in their use.]
Lege Artis Medicinae
FEBRUARY 21, 2004

[PRIMARY TUBULOINTERSTITIAL NEPHRITIS]
[Primary tubulointerstitial nephritis is characterised by an inflammatory infiltrate of tubulointerstitial space. The infiltrate consists of T and B lymphocytes, monocytes, macrophages, neutrophyl and eosinophyl granulocytes in varying degree. It is associated with interstitial oedema and different level of tubular damage. The disease exists in acute and chronic form. The main causes of this condition are: drugs, infection, systemic diseases, malignancy and in some cases the disease is idiopathic. The pathogenesis in most cases is immune-mediated. The secondary form of tubulointerstitial nephritis can occur in primary glomerular and vascular disease and is characterised by tubulointerstitial fibrosis and tubulus atrophy. The morphological alterations are major determinants of the progression of chronic renal disease. In both forms of tubulointerstitial nephritis the development of renal insufficiency is often observed.]
Lege Artis Medicinae
FEBRUARY 21, 2004

Lege Artis Medicinae
FEBRUARY 21, 2004
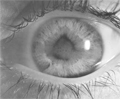
[EYE DISORDERS ASSOCIATED WITH MUSCULOSKELETAL DISEASES]
[The diseases of connective tissue and musculoskeletal system frequently associated with typical eye disorders. These can either be mild, recovering fully after treatment or more serious with persisting symptoms and destructive changes resulting in permanent loss of sight Eye symptoms can occur in the following diseases: rheumatoid arthritis, juvenile chronic arthritis, neonatal onset multisystem disease, ankylosing spondylitis, seronegative spondarthrities, Reiter’s syndrome, Behçet’s syndrome, Lyme disease, systemic lupus erythematosus, scleroderma, polyarteritis nodosa, Wegener’s granulomatosis, giant cell arteritis, erythema nodosum, relapsing polychondritis, sarcoidosis, Marfan’s syndrome, osteogenesis imperfecta.]
Lege Artis Medicinae
FEBRUARY 21, 2004
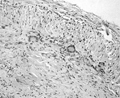
[LARGE VESSEL MANIFESTATION OF GIANTCELL ARTERITIS]
[The diagnosis of giant-cell arteritis is a real challenge for clinicians. There are several reasons for the difficulties in establishing the diagnosis. This disease is associated to rare conditions, therefore most physicians lack clinical experience. This condition shows very heterogeneous manifestation, the intensity of the symptoms vary in time. Early diagnosis is of great importance in order to prevent ischemic complications. Among these complications one should emphasise the role of anterior ischemic optic neuropathy that may result in abrupt blindness. In this case report, we show a rare socalled large vessel manifestation of giant-cell arteritis. This form of the disease needs different approach in diagnosis where color duplex ultrasonography may have distinguished importance. The final verification of the diagnosis is based on histology. However the lack of all histological criteria do not exclude the presence of giant-cell arteritis.]
Lege Artis Medicinae
FEBRUARY 21, 2004

Lege Artis Medicinae
FEBRUARY 21, 2004

[ACUTE DERMATOMYOSITIS ASSOCIATED TO THE CARCINOMA OF THE PROSTATE]
[INTRODUCTION - In some cases of polymyositis/ dermatomyositis (PM/DM) of autoimmune origin, different malignant tumours can initiate the difficult cascade mechanisms at cell level leading to the rapid weakness of the skeletal muscles. Till now, in the international literature only four cases of PM/DM associated with cancer of prostate has been reported. CASE REPORT - Authors present a case of a 57 yearold male patient, where weakness in patient's movements developed leading to total immobility in 3 months. Purple discoloration developed on his hand and face. Significantly elevated creatin kinase (CK) levels and blood sediment rate with mild anaemia were observed during laboratory examinations. Dysphagia and lack of appetite resulted in the loss 10 kgs in body weight. Both clinical evaluation, elevated serum CK level, skin symptomes, positive electromyography and muscle biopsy confirmed acute definitive dermatomyositis. Urological examination revealed a palpable hard area at the right lobe of the prostate. Prostate biopsy confirmed the presence of carcinoma in the right lobe of the prostate. There was no sign or symptome referring to either local propagation or distant manifestation. Therefore, radical prostatectomy was performed, the tumorous prostate and both seminal vesicles were removed. Histological examination proved malignant focus in the right lobe of the prostate. After the operation patient gradually became stronger, corticosteroid medication were decreased then stopped. Patient's original muscle power and movement recovered and his previous body weight was regained. During the regular control examinations all results of laboratory tests are in normal range. CONCLUSION - In the background of some autoimmune diseases malignant tumours can be revealed. It is rare when urological neoplasms initiative the process. In men with PM/DM commencing beyond 50 years of age it is necessary to think of the presence of prostate cancer, which can be cured by performing radical operation in appropriate time.]
1.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
2023 27. NOV
2.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
2023 27. SEP
3.
Clinical Neuroscience
Neuropathic pain and mood disorders in earthquake survivors with peripheral nerve injuries
2024 03. APR
4.
Journal of Nursing Theory and Practice
[Correlations of Sarcopenia, Frailty, Falls and Social Isolation – A Literature Review in the Light of Swedish Statistics]
2023 31. OCT
5.
Clinical Neuroscience
[Comparison of pain intensity measurements among patients with low-back pain]
2024 03. APR
1.
Clinical Neuroscience Proceedings
[A Magyar Stroke Társaság XVIII. Kongresszusa és a Magyar Neuroszonológiai Társaság XV. Konferenciája. Absztraktfüzet]
2024 06. SEP
2.
3.
Journal of Nursing Theory and Practice
[A selection of the entries submitted to the literary contest "Honorable mission: the joys and challenges of our profession" ]
2024 02. SEP
4.
Journal of Nursing Theory and Practice
[End of Life and Palliative Care of Newborns in the Nursing Context]
2024 02. SEP
5.
Journal of Nursing Theory and Practice
[Aspects of Occupational Health Nursing for Incurable Patients ]
2024 02. SEP