Bone-marrow transplantation (BMT), specifically hematopoietic stem-cell transplantation (HSCT) is a potentially curative treatment for a variety of malignant hematological diseases. Despite recent advances in this field, transplant-related severe medical complications, including graft-versus-host disease (GVHD) and mortality, remain serious and well-documented concerns1-4. As more sophisticated procedures have been developed and mortality rates have decreased over recent decades, attention has shifted to the psychosocial challenges associated with transplantation. Several studies have investigated psychological symptoms and quality of life (QOL) associated with HSCT5-9, but the studies were heterogeneous in terms of designs, patient populations, control groups, assessment tools, and time frames, thus yielded inconsistent findings. Studies on predictors have also yielded conflicting results regarding the impacts of socio-demographic factors, clinical variables (e.g., hematological disease type, transplant type, reduced intensity conditioning, and GVHD), and psychopathology on QOL following HSCT9–12. The conditioning regimen and transplant type have been reported to significantly impact the QOL and psychological symptoms of patients who have undergone HSCT13, 14. In studies comparing allogeneic HSCT and autologous HSCT recipients, similar or greater QOL impairments were observed in allogeneic HSCT recipients, and different recovery trajectories between the two groups were reported15–17. Conclusions drawn from the literature are limited by the heterogeneity of study samples, such as differences in age and pre-transplant comorbidities, higher rates of relapse in autologous transplant recipients, and the presence of GVHD symptoms in allogeneic transplant recipients. Numerous investigations have compared affective symptoms between patients undergoing allogeneic and autologous transplants, but the methodological diversity of these studies has also precluded drawing consistent conclusions14,18,19.
Post-transplant psychological morbidities, including depressive and anxiety symptoms, have been identified as major predictors of post-transplant QOL11,20. Most studies have reported moderate to severe depressive and anxiety symptoms in a large proportion of HSCT recipients21,22. A recent study that examined comorbidities in long-term survivors after allogeneic HSCT reported depression and anxiety among the most frequent comorbidities23. Interest in the relationship between clinically relevant depressive and anxiety symptoms and QOL is growing24. The most explored psychiatric conditions are major depressive disorder, generalized anxiety disorder, obsessive-compulsive disorder, and post-traumatic stress disorder25-27. Affective symptoms interfere with treatment adherence, adversely affect survival, and decrease patients’ perceptions of QOL9,20. Several studies have reported that GVHD is negatively correlated with QOL and psychopathology5,12,28. Patients with GVHD have a significantly impaired QOL, primarily in terms of physical and functional well-being5,17,29,30. The severity of chronic GVHD (cGVHD) has an independent negative association with QOL30-32; even mild cGVHD symptoms can decrease QOL below population norms30. A recent prospective study that examined the associations between psychosocial factors and QOL in cGVHD patients found clinically significant depressive and anxiety symptoms in approximately one-third of patients at different time points after HSCT. The HSCT symptom burden predicted depression symptoms, a poorer functional status predicted anxiety symptoms, and both were associated with QOL33. Patients with cGVHD and high levels of depression and anxiety constitute a highly vulnerable population for poor functioning, impaired QOL, and HCST-related mortality34.
The aim of this study was to compare the QOL and depressive and anxiety symptoms of patients after undergoing autologous or allogeneic HSCT to explore whether the HSCT type impacts on these aspects.
Our main hypotheses were that allogeneic transplant patients would have lower QOL scores than their autologous counterparts and that the QOL predictors would differ between the two patient groups. We predicted that severe clinical complications, such as acute/chronic GVHD and related poor health status, would be associated with poorer QOL after HSCT, and that allogeneic transplant patients would have more severe depressive and anxiety symptoms than their autologous counterparts.
Materials and methods
Participants
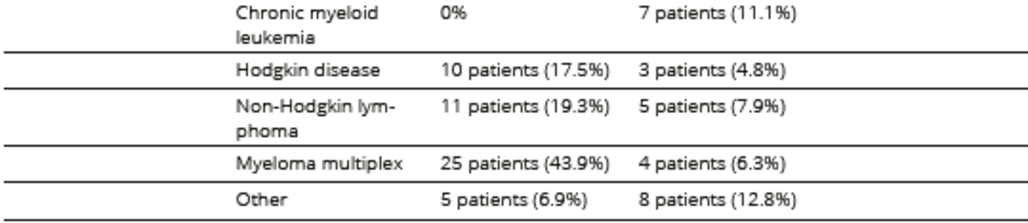
The study population comprised patients who were more than 18 years old with various hematological diseases, including acute and chronic lymphoid leukemia, acute and chronic myeloid leukemia, Hodgkin’s disease, non-Hodgkin’s lymphoma, and multiple myeloma, who underwent HSCT at the Bone Marrow Transplantation Unit, St. László Hospital (BMTU-SLH), Budapest, Hungary, between January 1, 1994 and December 31, 2008 and attended follow-ups at the outpatient service of the BMTU-SLH outpatient services. This cross-sectional study was conducted from March 2009 to May 2010. All outpatients at the BMTU-SLH were invited to participate by a research staff member. Participants were asked to complete the questionnaires while waiting for their routine follow-up examination.
The study protocol was approved by the Institutional Review Board of St. László Hospital. All participants signed a consent form before entering the study.
Assessment instruments
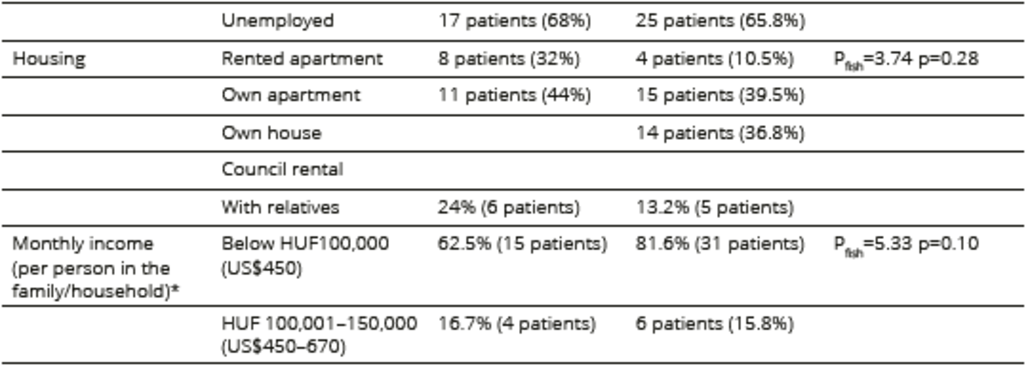
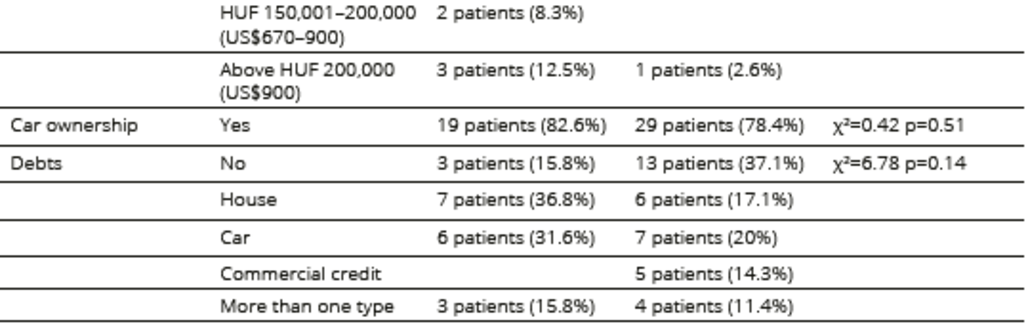
The participants’ basic sociodemographic data were collected using a self-reported questionnaire designed for this study with the following items: age, marital status, education, employment, place of living, type of accommodation, average monthly income, car ownership, and debt.
Clinical information, including the type and date of diagnosis and HSCT, type and severity of GVHD, disease status rated on a 3-point scale, treatment details, and the Clinical Global Impression (CGI) score (rated on a 7-point scale), was obtained from participants’ medical records or evaluated by their hematologists (CGI and disease status). Data on prior HSCT and psychiatric and medical history were also collected.
The Hungarian version of the Functional Assessment of Cancer Therapy–Bone Marrow Transplant Scale (FACT-BMT) was used to rate the participants’ QOL. The FACT-BMT is a 46-item questionnaire comprising five domains: physical, functional, emotional, and social well-being and BMT-specific complaints. The FACT BMT has good psychometric characteristics (Cronbach’s α = 0.89–0.94 for the entire test)35–37. Items were evaluated on a 5-point Likert scale, and higher scores reflect better QOL in each dimension. The overall QOL score was calculated by summing up the item scores.
Depressive and anxiety symptoms were assessed using the Beck Depression Inventory (BDI) and Spielberger’s State and Trait Anxiety Inventory (SSTAI), respectively. The BDI is a 21-item self-administered questionnaire. Each BDI item has four possible statements describing increasing symptom severity. Higher total scores indicate more severe depressive symptoms and syndrome (mild depression: 10–18; moderate depression: 19–25; severe depression: above 25)38,39. The SSTAI has “state” and “trait’” scales, each with 20 items. The “state” scale is used to determine the current level of anxiety, whereas the “trait” scale is used to detect the person’s “anxiety proneness”. Each question is rated on a 4-point Likert scale, amounting to maximum scores of 80 on each scale40.
Table 1. Sociodemographic characteristics of participants undergoing HSCT
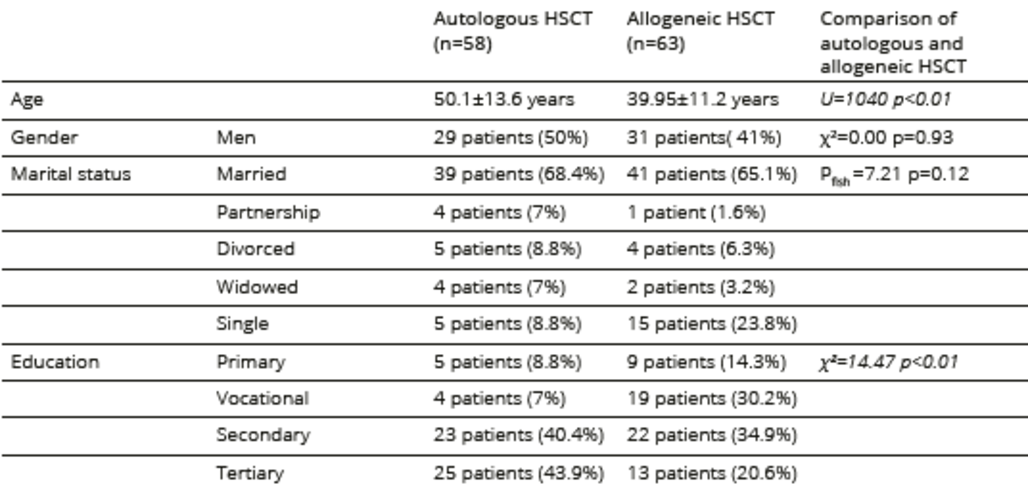
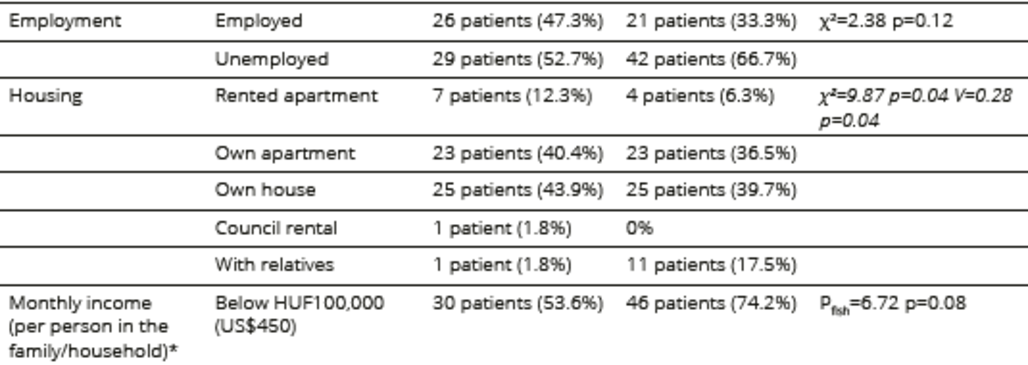
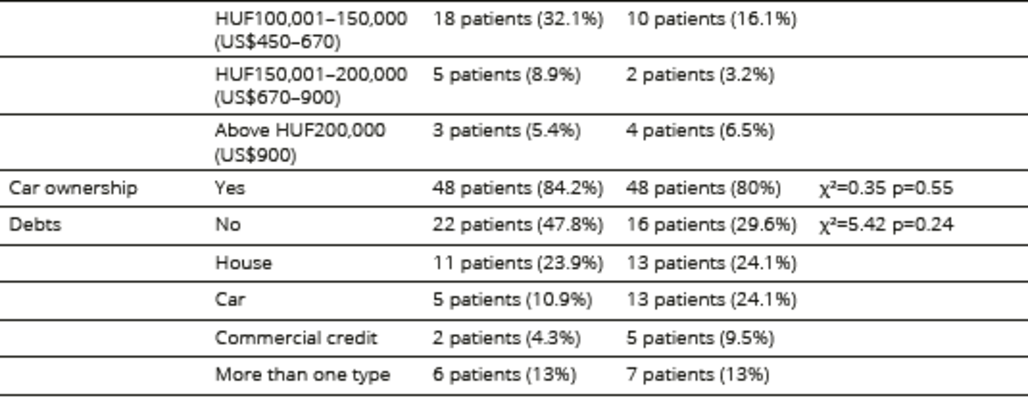
*date of currency exchange is 2012
Statistical analysis
Demographic and medical variables and FACT BMT, BDI, and SSTAI scores are presented as means and standard deviations or percentages, as appropriate. Correlations between the FACT-BMT, BDI, and SSTAI scores were analyzed using Pearson’s rho test when both variables were normally distributed and Spearman’s rank test when this criterion was not met. Comparisons between autologous and allogeneic groups were analyzed using a t-test when variables were normally distributed and a Mann–Whitney U test otherwise. Comparisons between groups with nominal variables were analyzed using Pearson’s chi-square test when the expected cell counts were not less than five and Fisher’s exact test or Cramer’s V otherwise. The Kolmogorov-Smirnov test was used to test for normal distribution.
A stepwise multiple linear regression analysis was conducted to identify factors that independently contributed to the total FACT BMT, BDI, and SSTAI scores in each group, which were the dependent variables. The independent variables were age, illness duration, medical or psychiatric comorbidities, time elapsed since HSCT, presence of acute or chronic GVHD, current treatment, stage of recovery, and the CGI score.
Results
Of the 258 HSCT patients who attended follow-ups at BMTU-SLH outpatient services during the study period, 208 (81%) were invited to participate in the study; 87 (23%) declined to participate, while 121 patients entered the study, constituting 32% of the eligible patient population (n=378) who had undergone HSCT. Reasons for non-participation included poor physical condition, impaired vision, lack of time, and a negative attitude toward psychological testing. The sociodemographic and disease-specific characteristics of the patient population are summarized in Tables 1, 2 and 3. Allogeneic patients were significantly younger than autologous patients. The time elapsed since HSCT was significantly longer in the allogeneic group, and more patients in this group considered themselves to be recovered or in remission. Patients who underwent allogeneic HSCT also received more immunosuppressive treatment related to acute and chronic GVHD symptoms than patients who underwent autologous HSCT.
The mean FACT-BMT score in the autologous cohort was 142.55 ± 25.50, with domain-specific scores of 20.91 ± 5.39, 17.55 ± 5.82, 21.47 ± 4.21, 19.14 ± 3.76, and 63.48 ± 15.44 for physical, functional, social, and emotional well-being and BMT-specific complaints, respectively. The mean FACT-BMT score in the allogeneic cohort was 142.13 ± 28.70, with domain-specific scores of 20.56 ± 5.89, 17.24 ± 7.21, 21.41 ± 5.06, 18.94 ± 4.90, and 63.98 ± 11.72 for physical, functional, social, and emotional well-being and BMT-specific complaints, respectively. The mean hematologic disease-related QOL scores in the autologous and allogeneic cohorts were 77.64 ± 17.16 and 77.90 ± 18.71, respectively.
The mean BDI scores in the autologous and allogeneic cohorts were 8.96 ± 5.50 and 11.05 ± 8.22, respectively, and the mean SSTAI scores were 80.72 ± 18.25 and 81.96 ± 21.24, respectively. The mean scores on the SSTAI Trait and State subscales were 41.11 ± 8.55 and 39.79 ± 11.24, respectively, for the autologous cohort and 42.76 ± 10.78 and 39.54 ± 12.00, respectively, for the allogeneic cohort. The BDI scores did not indicate depression in the autologous cohort and indicated only mild depression in the allogeneic cohort. Furthermore, the SSTAI scores in both cohorts corresponded to the anxiety level found in the general population40.
No significant differences in the mean FACT-BMT (p = 0.83), BDI (p = 0.24), and SSTAI scores (p = 0.69) were detected between the two groups.
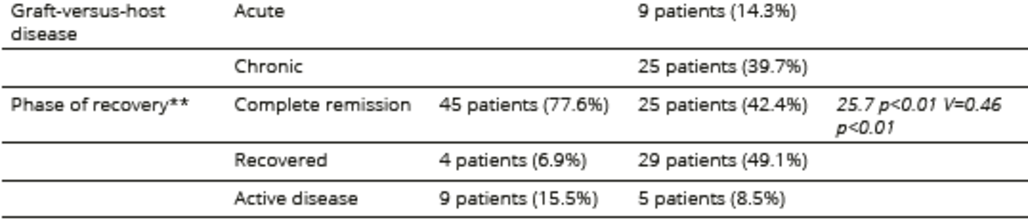
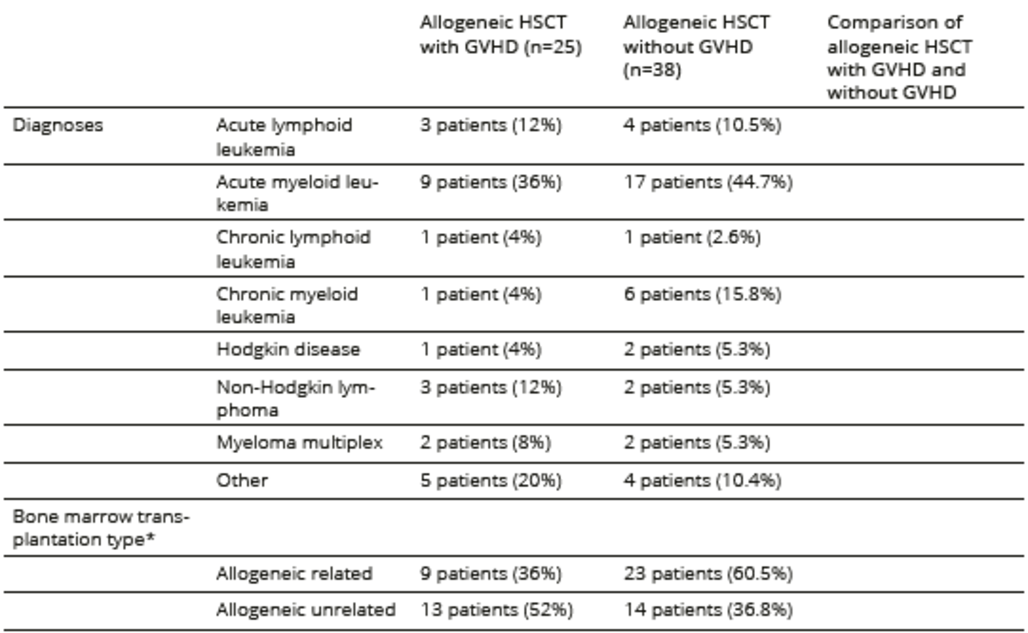
Table 2. Medical conditions related to the underlying hematological disease and treatment
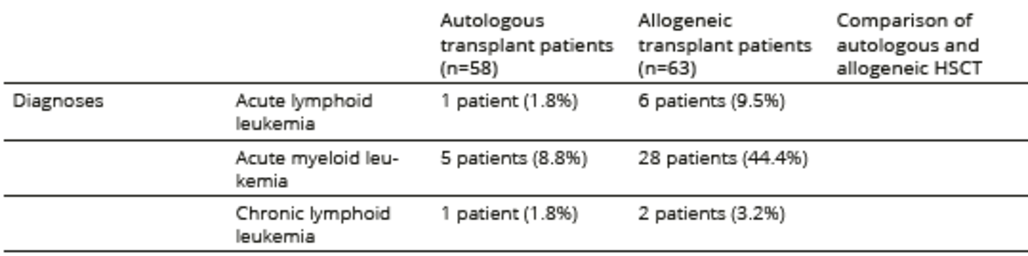
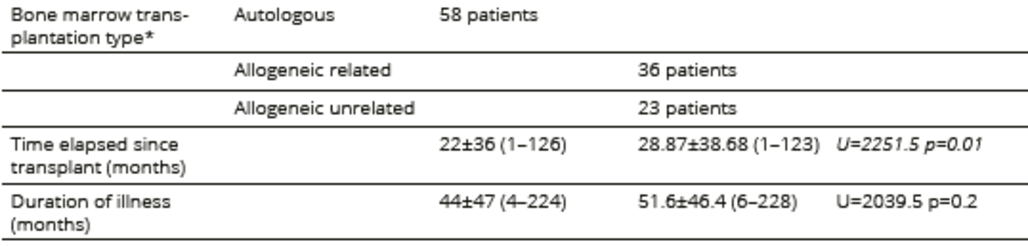

*type of transplant was missing in four cases in the allogeneic HSCT group
**phase of recovery data were missing in four cases in the allogeneic HSCT group
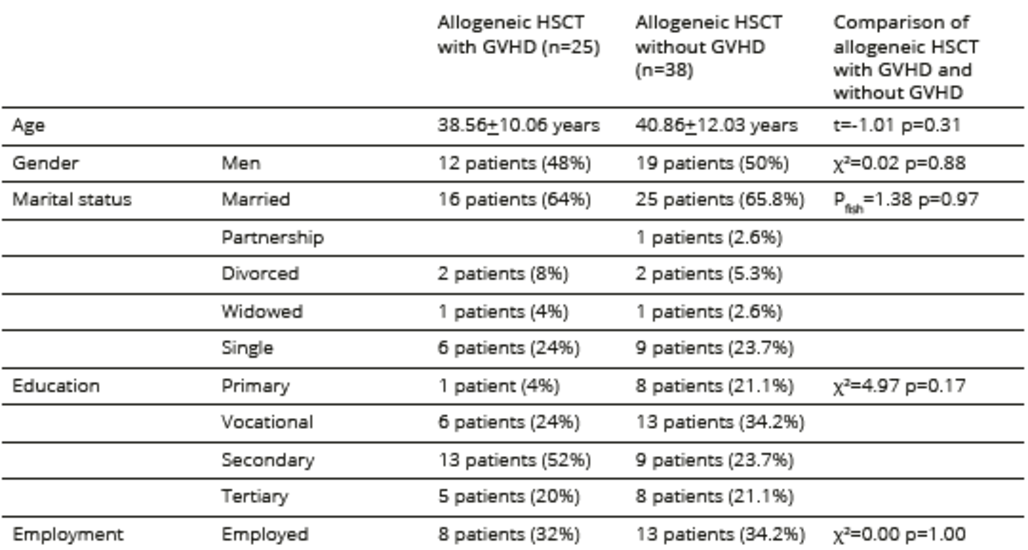
Table 3. Sociodemographic characteristics of participants undergoing allogeneic HSCT
*date of currency exchange is 2012
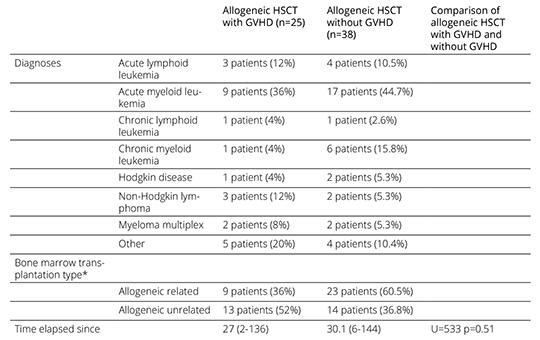
The comparison of allogeneic patients with and without GVHD symptoms revealed significant differences in the CGI (p < 0.01) and BDI (p = 0.01) scores. The SSTAI Trait Anxiety scores were significantly different (p = 0.04) between patients with and without GVHD. Among the domains surveyed in FACTBMT, a significant difference in BMT-specific items (p < 0.01), in FACT-GP scale (p < 0.05) and in total FACT-BMT (p < 0.05) scores was detected between the GVHD groups. No significant differences in sociodemographic and medical variables between patients with and without GVHD were found, excepting the immunosuppressive treatments. Allogeneic patients with GVHD symptoms received more immunosuppressive treatment than those without GVHD (Table 4). Comparisons between autologous and allogeneic patients without GVHD did not reveal significant differences in the FACT-BMT (p = 0.17), BDI (p = 0.77) and SSTAI (p= 0.25) scores. Comparisons between autologous and allogeneic patients with GVHD showed significant differences in the CGI (p < 0.01) and BDI (p <0.05) scores.
Table 4. Medical conditions related to the underlying hematological disease and treatment in allogeneic HSCT
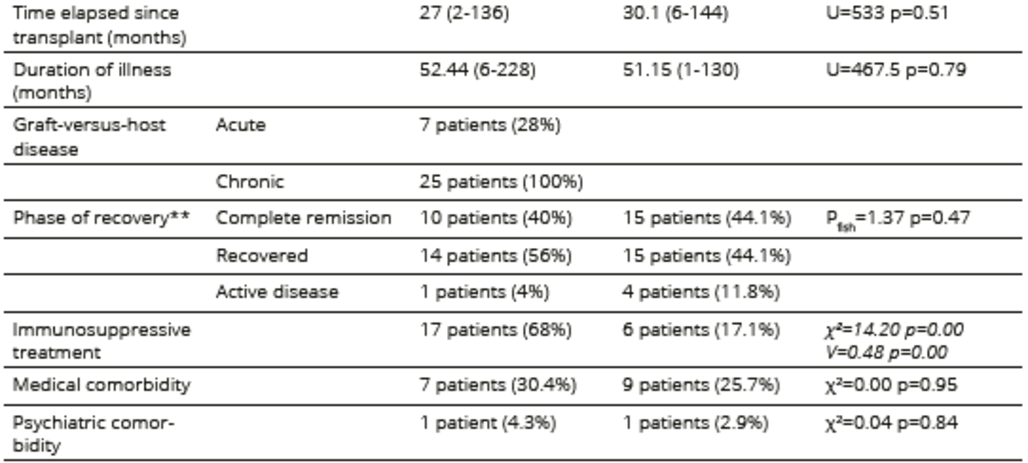
*type of transplant was missing in 3 cases in the allogeneic HSCT with GVHD and one case in the allogeneic HSCT without GVHD
**phase of recovery data were missing in four cases in the allogeneic HSCT without GVHD
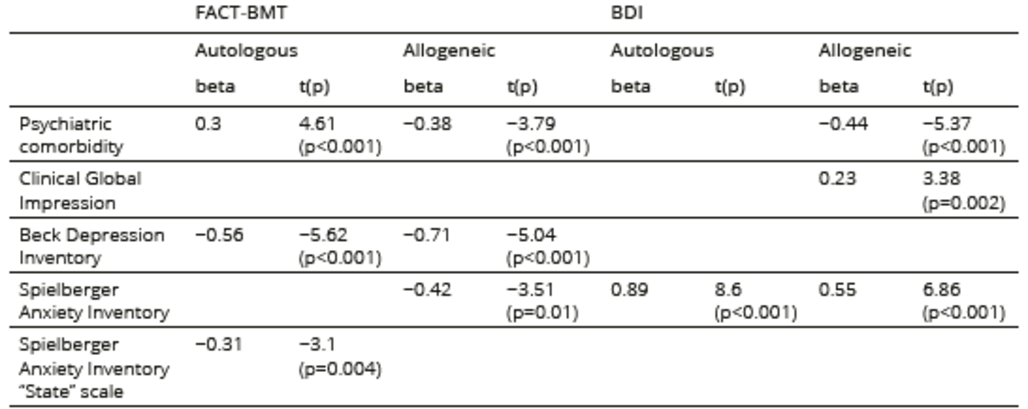
The stepwise multiple regression analysis revealed that psychiatric comorbidity, depression, and anxiety were significant contributors to QOL impairment in both the autologous and allogeneic groups. Poor QOL was independently associated with depression and anxiety in both groups. The contributors to depression were psy-chiatric comorbidity, anxiety, and CGI in the allogeneic group and anxiety in the autologous group. Functional deficit was independently associated with depressive symptoms in the allogeneic sample. The significant results of the multiple regression analysis are presented in Table 5.
Table 5. Variables independently associated with QOL and psychopathology (stepwise multiple regression analysis)
Discussion
This cross-sectional study found no direct impacts of the transplant type on the QOL or affective symptoms of patients. The main finding of the current study was that allogeneic transplant recipients with GVHD symptoms had a significantly poorer somatic status and more somatic complaints associated with transplantation and received more immunosuppressive treatments, impairing their QOL. Our results also indicated more severe depression with higher constant anxiety levels in patients with GVHD than those without GVHD, suggesting that GVHD significantly impacts the affective symptoms of allogeneic transplant patients through functional deficits and “somatic burden”. Our results confirmed the reported association between impaired QOL, symptom burden, and functional deficits derived from GVHD and affective symptoms in allogeneic recipients experiencing GVHD5,8,18,31,33. In earlier studies, depressive and anxiety symptoms were identified as significant risk factors for QOL deterioration after HSCT, indicating that depressed patients perceived their QOL to be poorer20,24. The present study confirmed this relationship in both allogeneic and autologous transplant patients, demonstrating that negative perceptions of QOL are independent of the transplant type. This negative perception among patients experiencing severe and enduring somatic symptoms caused by GVHD could increase the likelihood of depressive symptoms and, in turn, may influence different aspects of QOL. Comparisons between autologous and allogeneic patients with and without GVHD symptoms also allude to this association. Our findings indicate similar QOL and psychosocial functioning in autologous and allogeneic transplant patients without GVHD symptoms. Allogeneic transplant patients with GVHD symptoms had more depressive symptoms than autologous patients. Furthermore, allogeneic transplant patients with GVHD symptoms had worse QOL than those without GVHD symptoms. A longitudinal study is warranted to explore this association in depth.
These findings are consistent with the conclusion summarized in a previous paper34, showing that allogeneic patients with GVHD and depressive and anxiety symptoms constitute a highly vulnerable population for poor functioning, impaired QOL, and HCST-related mortality.
This study has methodological limitations that should be acknowledged. The main limitation was its cross-sectional design, which precluded investigation of the causality of associations between the risk factors in the trajectory of recovery. The sample size was also relatively small in view of the number and variety of clinical conditions that necessitate HSCT. As a clinical population, the study sample showed heterogeneity in certain aspects (age, psychosocial factors, medical variables), but these differences did not influence the results. Additionally, some data were missing for a few patients.




COMMENTS
0 comments