The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2006;59(11-12)
Content
Clinical Neuroscience
NOVEMBER 30, 2006




Clinical Neuroscience
NOVEMBER 30, 2006

[THE MODULATORY EFFECT OF ESTROGEN ON THE CAUDAL TRIGEMINAL NUCLEUS OF THE RAT IN AN ANIMAL MODEL OF MIGRAINE]
[Migraine is one of the most common neurological disorder affecting up to 14% of the population. The disease shows sexual dimorphism, thus gonadal steroids may play an important role in its patophysiology. One model of migraine headache is the systemic administration of nitric oxide (NO) donor nitroglycerin (NTG), which triggers a delayed attack without aura in many migraine patients but not in healthy volunteers. NTG is also able to activate the neurons of the caudal trigeminal nucleus in the rat. In our review we summarise the effect of NTG on the expression of some molecules, in the superficial laminae of the spinal portion of trigeminal nucleus caudalis, which play an important role in the pathomechanism of headaches, and the modulatory effect of chronic estradiol treatment. Our data show that NTG was able to modify all the examined substances in the caudal trigeminal nucleus, while chronic estradiol treatment abolished this effect. These data may help to understand the mechanisms by which estrogens influence trigeminal nociception and how nitric oxide triggers migraine attacks.]
Clinical Neuroscience
NOVEMBER 30, 2006

[ANIMAL MODELS OF HUNTINGTON’S DISEASE]
[Huntington’s disease is an autosomal dominantly inherited progressive neurodegenerative disorder. The main symptoms are choreiform, involuntary movements, personality changes and dementia. Huntington’s disease is a member of a group of diseases caused by CAG repeat expansions. One research aim is to determine the earliest molecular changes associated with Huntington’s disease. There is no possibility for this in humans, but various early changes have been identified in an animal model of Huntington’s disease. They are constructed by excitotoxin causing striatal lesion, or mitochondrial toxins inducing energy impairment, or by generating transgenic mice.]
Clinical Neuroscience
NOVEMBER 30, 2006

[CLINICAL ANALYSIS OF PATIENTS WITH PERIPHERAL FACIAL PALSY]
[symptoms. In two thirds of the cases the cause is unknown, this is called “idiopathic peripheral facial palsy or Bell’s palsy”, but several different diseases have to be considered in the differential diagnosis. In this paper we reviewed the case histories of 110 patients treated for “peripheral facial palsy” in the Department of Neurology, Semmelweis University, Budapest in a five year period, 2000-2004. We studied the age, gender distribution, seasonal occurance, comorbidities, sidedness, symptoms, circumstances of referral to the hospital, the initial diagnoses and therapeutic options. We also discuss the probable causes and consequences of diagnostic failures. Results: the proportion of males and females was equal. There was no considerable difference between sexes regarding agedistribution. Of the 110 patients 106 was diagnosed with idiopathic Bell’s palsy, three cases with otic herpes zoster and one patient with Lyme disease. In our material, peripheral facial palsy was significantly more frequent in the cold period of late autumn, winter, and early spring. Diabetes mellitus and hypertension were more frequent than in the general population. 74% of the patients were admitted within two days from the onset of the symptoms. In 37% preliminary diagnosis was unavailable. In 15% cerebrovascular insult was the first, incorrect diagnosis, the correct diagnosis of “Bell’s palsy” was provided only in 16%. The probable causes of diagnostic failures may be the misleading symptoms and accompanying conditions. We examined the different therapies applied and reviewed the literature in this topic. We conclude that intravenous corticosteroid treatment in the early stage of the disease is the therapy of choice.]
Clinical Neuroscience
NOVEMBER 30, 2006

[AMYOTROPHIC LATERALSCLEROSIS IN COUNTY BARANYA, HUNGARY]
[Amyotrophic lateralsclerosis is a progressive neurodegenerative disease resulting in loss of upper and lower motoneurons. Here we analyzed the clinical and epidemiological data of 202 ALS patients admitted to our department between 1950 and 2004. Risk and protective factors influencing onset and progression of the disease were examined. We also analyzed the relationship between first clinical symptoms/signs and prognosis of the disease. Our data suggest the importance of toxic factors in the initiation of the disease and the effect of clinical phenotype on the progression of ALS.]
Clinical Neuroscience
NOVEMBER 30, 2006

[NEW METHODS IN THE INVESTIGATION OF BRAIN HYPOXIA]
[The main challenge is the investigation of mechanism for apoptosis research and the drug development. Mitochondria have a key position in the production of reactive oxygen species and in the evolution of apoptosis. More possible pathway will be known with the apoptosis investigation. For development of neuroprotective molecules could give strategies the investigation of apoptosis. Exact knowledge of apoptosis provides possibility to screen new neuroprotective molecules. We elaborate a research assay, which could provide quantitative and qualitative data about the free radical production and the mitochondrial transmembrane potential using confocal microscope. So thus we could screen drug candidate, neuroprotective molecules.]
Clinical Neuroscience
NOVEMBER 30, 2006

[MOVEMENT-RELATED BETA RESPONSES IN ESSENTIAL TREMOR AND PARKINSON’S DISEASE]
[Objective - To investigate the pathomechanism of essential (ET) and parkinsonian tremor (PT) by studying the correlation between tremor severity and movement-related beta rhythm changes of the human electroencephalogram. Patients and methods - We recorded the electroencephalogram of 10 patients with essential tremor, 10 with Parkinsonian tremor and 10 controls. In a preliminary session we determined the side with lower and higher tremor intensity (T+, T++ respectively), using accelerometry. Subjects pressed an on-off switch in a self-paced manner with left and right thumb. After digitalization of the EEG from Cz, C3, C4 electrodes, the movement reactive beta frequency (MRBF), its minimum/maximum peak power values and their latencies triggered to movement offset were determined. Results - The time course and amplitude of movement related beta desynchronization (ERD) were similar in each group regardless of tremor intensity. In ET tremor severity did not influence post-movement beta synchronization (PMBS) amplitude (PMBSET+=100.98±48.874%, PMBSET++=135.1±92.87%; p=0.231), however it was significantly delayed after the movement of the more tremulous hand (latPMBSET+=1.26±0.566 s, latPMBSET++= 1.57±0.565 s, p=0.003). In the PT group on the side of pronounced tremor the amplitude of PMBS decreased but it was not delayed, compared to the less affected hand (PMBSPT+=115.19±72.131%, PMBSPT++= 77.84±53.101%, p=0.0028; latPMBSPT+=1.4±0.74 s, latPMBSPT++=1.25±0.797 s, p=0.191). In controls the power and latency of PMBS was similar on both sides. Conclusions - The results suggest that neuronal mechanisms underlying PMBS generation are differently affected by ET and PT. Investigation of PMBS might be used for the differential diagnosis of essential tremor and Parkinson's disease.]
Clinical Neuroscience
NOVEMBER 30, 2006

[BIOMECHANICS OF INTRACRANIAL ANEURYSMS]
[Introduction - Viscoelastic parameters of circumferential and meridional strips of ruptured and silent aneurysms were investigated (considered clinical and histological data either) in order to advance the prediction of risk of aneurysm rupture. Method - In our clinical practice, aneurysms managed by microsurgery aneurysm clipping were removed. Meridional and circumferential strips were cut. Strips were investigated by an uniaxial biomechanical instrument: distending force was recorded as the length of the strips was increased in steps. Normal stress-relaxation patterns were detected. The shape of strain curves well overlapped with the Standard Linear Solid Model curve, as had been expected. The viscosity, serial and parallel elastic moduli of the model were then computed. Results - Linear correlation was demonstrated amongst peek distending force detected and aneurysm strip thickness. Steric inhomogenity was detected at the meridional and circumferential strips. Strain-stress behaviour of ruptured and silent aneurysm specimen showed significant difference. Values of strips originated from patients suffered from hypertension as well as strips originated from aneurysms had been histologically found inflamed were higher. Discussion - Results of these observations are going to be used to set three dimensional computer model in cooperation with IT team of Budapest University of Technology and Economics to advance rupture risk prediction.]
Clinical Neuroscience
NOVEMBER 30, 2006
[COMPLEX NON-INVASIVE HEMODYNAMIC SYSTEM FOR THE EVALUATION OF VASCULAR STATUS]
[The vascular diseases (myocardial infarct, stroke, peripheral occlusive disease) have a common pathophysiological background, the arteriosclerosis, that impairs the autoregulation of cerebral vessels, decreases the endothel mediated flow in the peripheral vessels. Therefore the assessment of the vascular damage or the follow-up of therapy need a complex and simultaneous approach. Currently the morphological and functional changes in the vascular system can be investigated with separated measuring systems, focusing either to cardiac or cerebral parameters (intermittent blood pressure measurement, ECG, cerebral blood flow by transcranial Doppler e.g.). Our purpose is to establish a complex non-invasive system for the simultaneous measurement and comparison of cardiac/cerebral/periheral hemodynamics. The hemodynamic parameters in hypertensive patients are examined with transcranial Doppler and cardiac monitoring during tilt-table test. Intima-media thickness, flow-mediated dilatation in brachial artery, augmentation index and pulse wave velocity are also measured. The measurement will be repeated after 6 and 12 months follow-up. Our preliminary results are similar to those found in the literature, that proves the reliability of our complex noninvasive hemodynamic system. It is assumed, that 12 months antihypertensive therapies with ACE inhibitors, calciumantagonist etc. might result in different effects on different vascular parameters. Our system enables the individualization of antihypertensive therapy.]
Clinical Neuroscience
NOVEMBER 30, 2006

[THE ROLE OF TREMOROMETRY IN PREDICTING THE OUTCOME OF ABLATIVE SURGERIES]
[Ablative neurosurgical interventions are widely used for the treatment of advanced Parkinson's disease. However, in some cases, the achieved result is temporary and repeat operation is necessary to obtain a permanent effect. By analyzing 30 ablative surgeries using comparative accelerometry, we looked for a biological marker predicting the efficiency. In 27 cases where clinical symptoms were permanently improved, a significant increase in rest tremor frequency was observed in addition to reduction in tremor intensity. In contrast, in those three cases where the clinical effect of the surgery was only temporary, the frequency of tremor remained unchanged despite of the transitory decrease in intensity. We thus hypothesize that postoperative change in frequency of tremor but not the intensity may predict the outcome of ablative treatments.]
Clinical Neuroscience
NOVEMBER 30, 2006
[LONG-TERM APPLICATION OF THE MULTIPLE SCLEROSIS FUNCTIONAL COMPOSITE IN DEBRECEN]
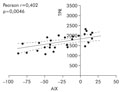
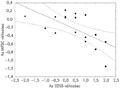
[Introducion - The multiple sclerosis functional composite (MSFC) has been recommended by the National Multiple Sclerosis Society as a new clinical outcome measure. It is based on measurements in three clinical dimensions: leg function/ambulation (timed 25-foot walk), arm function (9 hole peg test) and cognitive function (paced auditory serial addition test). Scores on component measures are converted to standard scores (Z-scores), that reflect patient performance. This method has not yet been introduced into routine clinical practice. Patients and methods - Since March 2000 over the five years period the MSFC calculation was applied to 17 patients with relapsing-remitting multiple sclerosis (age mean: 37.4±10.8 years, duration of the disease: 5.5±4.9 years, EDSS: 2.7±1.4) seen at the neuroimmunological outpatient clinic to evaluate its usefulness and its correlation with the traditionally applied expanded disability status scale (EDSS). Thirteen patients received immunomodulatory treatment (interferon beta and glatiramer acetate), one patient received immunosuppressant therapy (azathioprine), and there was a patient, to whom developed secondary - progressive phase and we changed the interferon treatment to mitoxantrone. MSFC and EDSS were measured at 3., 6., 9, 12., 18 and 60 months of follow-up. Results - The prospective study confirmed a strong correlation between EDSS and MSFC in multiple sclerosis. The MSFC was more sensitive to clinical changes than EDSS. Our results after 18 months of follow up are already published. After five years arm/hand function and leg function/ambulation were the most sensitive mesures for disease progression. In contrast with the literature we did not experience correlation with cognitive changes. Consequences - We demonstrated strong correlation between MSFC and EDSS after a longer period. MSFC is a simple method, suitable for follow-up of multiple sclerosis patients in everyday clinical practice.]
Clinical Neuroscience
NOVEMBER 30, 2006

[EPIDEMIOLOGY OF STROKE IN THE ELDERLY]
[Background - In the industrialized countries the very elderly stroke patient is more frequent than before. For the time being Japanese people have the highest expected lifespan, so the epidemiological features of stroke in the very elderly can be examined here quite easily. From a few publications with low case number it is known that in this group of patients the statistical characteristics of stroke is remarkably different from the youngers' one. Subjects and methods - The subjects aged 85 or more years were selected from the Akita Stroke Registry with first-ever acute stroke from 1996 to 1998. Results - 8,046 cases were recorded. There were 7362 patients aged <85 years, and 684 patients aged ≥85 years (8.5%). Sex ratio (women/men) was 1.89 in the two age groups. In the population of Akita the crude incidence of firstever stroke was 222/100,000/year, and 1,085/100,000/year in the very elderly, who were characterized with relatively lower prevalence of stroke risk factors, except that of atrial fibrillation (26.9%) and cardiac diseases (34.2%). The stroke subtype distribution (cerebral infarction 73.2%, intracerebral haemorrhage 20.6%, subarachnoidal haemorrhage 6.1%) was significantly different from the one known in Japan. Mortality rates were considerably high, especially in the SAH group. The most powerful prognostic factor of death was the consciousness level at onset. The following in order of predicting value was the SAH stroke subtype. Conclusion - While people aged 85 years or more had relatively lower prevalence of cardiovascular risk factors, they suffered stroke with very high frequency, the evolved cerebrovascular event caused very severe symptoms and led to death with high rate. Implicitly this is illuminating the complexity of aging as a procession, furthermore it raises the importance of prevention, more rather of the acute stroke care and rehabilitation in this high age group.]
Clinical Neuroscience
NOVEMBER 30, 2006

[THORACIC MENINGOCELE]
[Herniation of the meninges through a defect of the spinal canal is a spinal meningocele, and is usually located dorsally in the lumbosacral region. Meningoceles are usually part of a complex developmental disorder, or of a systemic disease, or it can be iatrogenic, as well. We report a very rare case of a true anterior thoracic meningocele.]
Clinical Neuroscience
NOVEMBER 30, 2006

Clinical Neuroscience
NOVEMBER 30, 2006

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.