The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Hungarian Radiology - 2002;76(03)
Content
Hungarian Radiology
JUNE 20, 2002




Hungarian Radiology
JUNE 20, 2002

[MR-guided ultrasound surgery]
[The powerful union of focused ultrasound surgery and magnetic resonance imaging has created a new approach to noninvasive surgery. Using this integrated therapy delivery system the physician can achieve correct localisation of tumors, optimal targeting of acoustic energy, real time monitoring of energy deposition, and the means to accurately control the deposited thermal dose within the entire tumor volume. The advantages of MRI over ultrasound guidance in controlling focused ultrasound surgery lie in the more sensitive detection of tumor target, the real time detection of tissue temperature, and the confirmation of thermally-induced tissue changes - powerful features that eventually can replace the traditional surgical approach. Applying software that connects the therapy and imaging system, the physician can generate an entire plan from quantifying temperature changes to positioning the therapy transducer. The non-invasive debulking of tumors without disturbing adjacent, functionally intact structures is thereby accomplished. Ongoing clinical trials involving the treatment of breast fibroadenoma, localized breast cancers, and uterine fibroids have been most encouraging. But nowhere has the application of MRI-guided focused ultrasound surgery been more compelling than in brain, where not only tumor treatment is possible but also the focal, transient, reversible breakdown of the blood-brain-barrier. The implications of this mechanism for targeted intra-cerebral tumor therapy or other non-oncologic applications are clearly enormous. In addition to tumor treatment, MRI-guided focused ultrasound surgery has other potential clinical applications such as vascular occlusion, targeted drug delivery, and targeted gene therapy. FUS is not a new idea but the emergence of MRI based guidance has accelerated the progres of focused ultrasound surgery technology, certain weaknesses remain including excessively long treatment times, body and organ motion, and difficulties in finding acoustic windows at certain anatomic locations. Nevertheless, the successful clinical implementations of this method is already in progress.]
Hungarian Radiology
JUNE 20, 2002
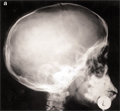
[Chondrodysplasia punctata - retrospective diagnosis]
[A 10 year-old, mentally normal boy with flat face, skin abnormalities, contracture of Achilles and knee tendons, strabismus and unique bony abnormalities is reported. The characteristics of skin changes and pattern of bony abnormalities allowed the retrospective diagnosis of atypical form of chondrodysplasia punctata.]
Hungarian Radiology
JUNE 20, 2002
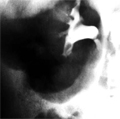
[Ogilvie’s syndrome associated with excretory urography]
[INTRODUCTION - The Ogilvie's syndrome is a disturbance of colonic innervation with parasympathic overreaction was assumed to be cause of large bowel segment spasm and poststenotic accumulation of gas. There is no distention in small intestine. CASE REPORT - In case of a 15 years old male during excretory urography six minutes after the administration of contrast material infusion Ogilvie's syndrome had occured. On 6, 12 and 18 min. abdominal plain film were demonstrated the acute spasm and poststenotic large bowel distention by air lumenogram phenomenon in the kidneys ambilateral renal tuberculosis by the whitening-like contrast opacity arising from centre calyx (pyelotubular reflux) in right side and by clubbing of calyces in left side (daisy flower sign). Not involved the small intestine. The colonic spasm and accumulation of gas lasted approximately 6 hours and ceased without medical aid. CONCLUSION - The Ogilvie's syndrome accompanying excretory urography is a toxic effect attributing to transient injury of peripheric neures and neurovisceral synapses.]
Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002
Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002

Hungarian Radiology
JUNE 20, 2002

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.