The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Oncology - 2020;7(3)
Content
Clinical Oncology
AUGUST 28, 2020




Clinical Oncology
AUGUST 28, 2020
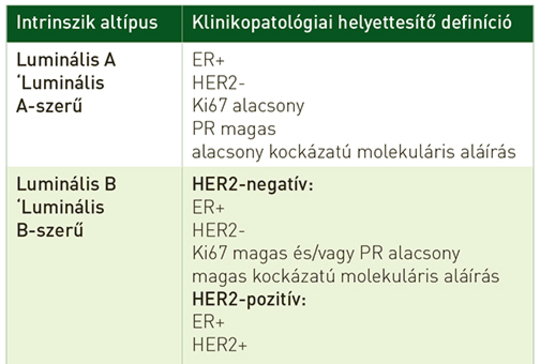
[The hormonal therapy of breast cancer]
[Breast cancer will be diagnosed in 12% of women in well-developed countries over the course of their lifetimes. This review focus on current approaches and strategies of systemic endocrine therapy of breast cancer. Breast cancer can be divided into three main subgroups based on the presence and absence of molecular markers (ER, PR, HER2 receptors). For patients without metastases the therapeutic goals are preventing the locoregional and distant recurrence. The length of adjuvant hormonal treatment is an important question in the everyday oncological practice. For patients with metastatic breast cancer the goal of the therapy is prolonging life, keep quality of life and palliating cancer symptoms. Patients with hormone receptor positive (HR+) tumours receive endocrine therapy, in monotherapy or in combination. As the result of new therapeutic approaches and of international drug development, HR+ breast cancer patients have more and more therapeutic options in case of early breast cancer as well as in metastatic settings.]
Clinical Oncology
AUGUST 28, 2020
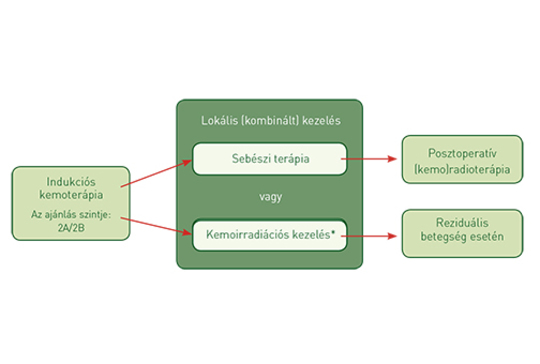
[Complex treatment of head and neck cancers – overview]
[Treatment of head and neck squamous cell carcinomas (HNSCC) is exceptionally complex, requiring the close cooperation of the head and neck surgeon, radiation oncologist and medical oncologist. Excellent tumor control should be our primary goal, however, the selection of treatment should not only be guided by oncologic radicality but by the need of satisfactory quality of life (as most local therapies affect respiratory, swallowing and/or speech function), too. Based on the appropriate diagnostic workup, these cancers are classifi ed into early, locoregionally advanced or recurrent/metastatic stages. Each category requires different treatment modalities, further complicated by the localization of the primary tumor and its metastases, performance status of the patient, comorbidities, and the biology of the lesion. In the present review, the authors summarize the basics of the therapy of head and neck cancers.]
Clinical Oncology
AUGUST 28, 2020
Clinical Oncology
AUGUST 28, 2020
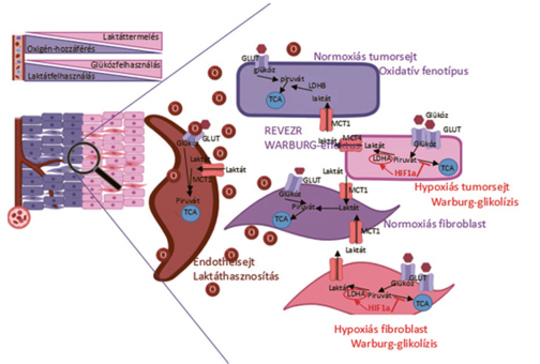
[Importance of hypoxia in tumor progression: road to Nobel price and novel therapeutic opportunities]
[It is now evident that cancer hypoxia is one of the new hallmark of cancer due to its consequences in gene expression, metabolism and biology. The importance of cancer hypoxia was recognized by the Nobel-price award in 2019. There are three major causes of cancer hypoxia: insuffi cient vascularization, systemic hypoxia of the host and constitutive activation of oncogene driven signaling pathways, all leading to a unique form of genetic reprogramming by HIF transcription factors. The consequences of HIF activation in cancer is the angiogenic phenotype, a new metabolic profi le and an immunsuppressive microenvironment. Furthermore, cancer hypoxia and the cellular adaptation lead to therapy resistance. Accordingly there is an urgent need to develop target therapies of hypoxia to improve effi cacies of various therapeutic modalities.]
Clinical Oncology
AUGUST 28, 2020

[The use of vitamins and trace elements in oncology]
[The effects of diet on development cancer and tumor control has been studied for along time, because diet has a key role in treatment of cancer. A multidisciplinary team is needed for proper use of vitamins and trace elements in cancer patients. This multidisciplinary team (oncologist, dietitian, laboratory assistant) can provide the professional supervision from the medical examination to the practical implementation, which can control the proper intake of these nutrients and the individual conditions. Dietetian is helped by appropriate health assessment (blood testing, gut microbiome and nutrigenetics) and targeting to determine the accurate amount and methods (food or dietary supplements) of vitamins and trace elements. Dietitans can help the patients to analyze the nutrients intake by food, determine the needs of the nutrients, and implement the results in practice.]
Clinical Oncology
AUGUST 28, 2020
[The indication for surgical resection in secondary liver malignancies - New therapeutic approaches]
[During the last decade liver surgery underwent major improvement: mortality rates reduced meanwhile new surgical approaches converted surgeons’ consideration on many advanced cases likely to be resectable. Liver is the most frequent site for tumor metastases and liver metastasis surgery experienced major changes as well. As long as liver resection related mortality rates have decreased indication for operative treatment of liver metastasis with certain primary tumors (stomach, pancreas) gained reconsideration and became reasonable. New surgical methods and approaches (laparoscopy, portal vein embolization) came into everyday application meantime several researches were completed enabling oncological aspect interpretation. Laparoscopy is a proven rational way of approach not only in cases of primary but metastatic liver tumors too: short and long term survival rates and oncological results are comparable with the results of open surgery. Although reports on large number series have not yet been published, it seems that practice of laparoscopy can bring increased number of cases where resection of primary tumor and synchronous liver metastasis can be performed simultaneously. Treatment strategies including surgical procedure overwhelm results of schemes planned with chemotherapy lines only even for patients suffering from advanced metastatic disease with necessary extended liver resection together with major vessel resection or for those who require liver resection following portal occlusion method. Consent opinion in best therapeutic option by oncologist and surgeon is essential to reach optimal liver metastasis patient treatment.]
1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.