The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2009;62(05-06)
Content
Clinical Neuroscience
JUNE 02, 2009

[Pain sensitivity changes in schizophrenic patients and animal models - Part II.]
[Diminished pain sensitivity in schizophrenic patients has been reported for more than 50 years, however little is known about the substrate and the basic mechanisms underlying altered pain sensitivity in this disease, therefore, relevant animal models are of decisive importance in the study of psychiatric diseases. The authors report a review consisting of two parts focusing on pain sensitivity changes in patients and in different animal models which proved the eligibility as schizophrenia models and pain sensitivities have also been determined. The second part of this article analyzed the results regarding knock out mice as schizophrenia models. These data proved that several genes have significant role in the pathomechanism of schizophrenia; therefore deficiency in one gene does not produce animals showing all signs of this disease. As regards the pain sensitivity changes, only a few data are available with controversial results. Data originated from complex chronic animal models indicate that they might be more adequate methods for studying the mechanisms of schizophrenia including the pain-sensitivity changes.]



Clinical Neuroscience
JUNE 02, 2009

[Genetics and present therapy options in Parkinson’s disease: a review]
[In the past years, six monogenic forms of Parkinson disease have clearly been associated with this movement disorder. The most frequent forms are LRRK2- and Parkin-associated Parkinson disease. Currently, a genetic diagnosis does not change the therapy, the genes involved in genetic Parkinson disease help to understand the underlying pathophysiologic mechanisms of Parkinson disease. Beside the overview of the molecular-genetic basis, we give a review about genetic testing, pharmacological and other multidisciplinary treatment options.]
Clinical Neuroscience
JUNE 02, 2009

[Hypertension and it’s therapy in acut phase of stroke]
[The elevation of blood pressure above normal and premorbid values within the first 24 hours of symptom onset in patients with stroke is relatively common. This acute hypertensive response is usually managed by different group of physicians, including general practitioners, emergency physicians, neurologists, internists, intensivisists. Management strategies of this phenomenon vary considerably. The first consideration in blood pressure management in this clinical setting is to determine whether the patient might be a candidate for thrombolytic therapy. For those patients are not entitled to that therapy premorbide blood pressure values and the type of stroke are the key data for sufficient control of hypertension. In patients with chronic hypertension, the lower end of the autoregulation curve is shifted toward high pressure and an impaired autoregulation due to acute stroke may increase the risk for further brain tissue damage if the blood pressure is inadequately controlled. The current guidelines recommend lowering blood pressure in patients with an intracranial haemorrhage below 160- 180/100-105 mmHg, if the patient is normotensive, while the target level is 180/105 mmHg in hipertensive patients. However, in ischaemic stroke no treatment is recommended if systolic blood pressure <220 mmHg and/or diastolic blood pressure <120 mmHg in the acute stage. Clinical studies are rare which assess the effectiveness of different antihipertensive drugs in acute stroke. The first strong evidence came from the ACCESS (The Acute Candesartan Cilexetil Therapy in Stroke Survivors) trial which suggested that a 7-day course of candesartan after an acute ischaemic stroke significantly improves cardiovascular morbidity and mortality.]
Clinical Neuroscience
JUNE 02, 2009

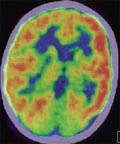
[99-mTc-HMPAO single photon emission computed tomography examinations in genetically determined neurometabolic disorders]
[The aim of our study was to determine regional cerebral blood flow (rCBF) abnormalities in different types of enzymopathies. Patients and methods - Among the patients with genetically determined enzymopathies 3 patients had aminoacidopathies, and 11 had different types of encephalopathies, from which 10 had mitochondrial encephalomyopathy (MEMP), and 1 patient had hyperuricaemic encephalopathy. Besides the mentioned 14 patients, 1 had ceroid lipofuscinosis and another patient had tuberous sclerosis. The further distribution of the MEMP patients’ group was the following - 5 patients had MEMP with lactic acidosis, 5 had Leigh’s disease (subacute necrotizing encephalopathy), from which 1 had cytochrome-c-oxidase deficiency (COX). Additionally in all patients were performed cerebral MRI and SPECT examination 10 min. after intravenous administration of 20 Mbq/kg 99 mTc-HMPAO. Results - Fourteen out of 16 SPECT findings were pathologic, showing decreased focal frontal/temporal/temporoparietal cerebral blood perfusion. Aminoacidopathic group - all the 3 patients revealed pathologic signs from the aminoacidopathic patients’ group. Among them the ornithine transcarbamylase (OTC) heterozygous female patient with left-sided hemiparesis caused by hyperammonemic stroke at 10 month-age, showed right sided temporoparietal, occipital and left frontal hypoperfusion, nearly 6 years after the cerebral vascular attack. This finding might be resulted because of diaschisis. Mitochondrial encephalo-myopathic (MEMP) group - all the four patients with MEMP and lactic acidosis showed focal hypoperfusion in the temporal region, while the perfusion was normal in the COX deficient patient and in 2 Leigh’s disease (subacute necrotizing encephalopathy) patients. In the remaining 1 Leigh’s patient frontotemporal hypoperfusion was found. In all patients there were non specific structural abnormalities detected by MRI - cortical and subcortical atrophy, and scattered demyelination foci. In the case of ceroid lipofuscinosis the MRI showed cerebral atrophy and cerebellar hypoplasia, and the SPECT showed right frontal and occipital hypoperfusion, bilateral parietal physiological riping process. The patient with tuberous sclerosis showed bilateral temporo-occipital hypoperfusion. Conclusion - 1. SPECT images demonstrated hypoperfusion rCBF changes in 14 out of all 16 patients. 2. Regional cerebral/cerebellar hypoperfusion was detected by SPECT in mitochondrial encephalomyopathies, with lactate acidosis and aminoacidopathies giving high informative value about the cerebral perfusion.]
Clinical Neuroscience
JUNE 02, 2009

[Long term experience with Stalevo]
[The triple combination of levodopa, DDCI and entacapone (Stalevo) is used to treat motor complication in patients with Parkinson,s disease. In this study we summarized the clinical data of our patients treated with Stalevo for the longest period. We can concluded, that after switching to Stalevo due to wearing off, the average levodopa doses were lower then before and the motor complications were milder. After 3 years of Stalevo therapy the levodopa doses were increased but still did not reach the average doses before introducing Stalevo. After switching the patients, general well-being was improved as indicated by the visual analogue scale. In summary, the Stalevo treatment is safe and effective for long run and improves the patients, quality of life.]
Clinical Neuroscience
JUNE 02, 2009
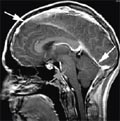
[Severe intracranial hypotension in an adolescent with Marfan syndrome. Case report]
[Spontaneous intracranial hypotension is a rare complication of connective tissue disorders. One of them is Marfan syndrome. It predisposes the patient to meningeal diverticula. Possibly after minor unrecognised head trauma or secondary to Valsalva manoeuvre cerebrospinal fluid leak from meningeal diverticula can happen. It causes postural headache. We describe a 15 year old adolescent female newly diagnosed with Marfan syndrome, who presented with intractable postural headache. Our patient's brain MRI showed bilateral frontal subdural effusion, narrow ventricles, downward displacement of the brainstem, enlarged cervical venous plexi, dural ectasias and wide nerve root sleeves. Radionuclide cisternography demonstrated CSF leaks at multiple sites. She could not be treated conservatively, but was successfully treated by epidural saline injections. Control brain and cervical MRI confirmed her healing, too. At the two and half year follow up visit, she was completely well. So we recommend this easiest technic to use before epidural autolog blood patches.]
Clinical Neuroscience
JUNE 02, 2009
[Surgically cured resistant epilepsy - caused by hemispherical dysgenesis - Case report]
[A part of patients with the therapy resistant epilepsy can be cured by surgical interventions. The more concordant the presurgical evaluation data, the better prognosis the patient has postoperatively. In case of discordant examination data, multimodal evaluation or case-specific decision might be successful. We report on a five-year-old boy with bilateral (left-dominated) cortical dysplasia and therapy resistant epilepsy. The ictal EEG did not help to localize the seizure onset zone, semiology had little lateralization value; however, FDG-PET showed left hemispherial hypermetabolism. The child became almost seizure-free and showed improved development after left-sided hemispherotomy.]
Clinical Neuroscience
JUNE 02, 2009
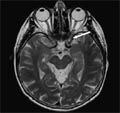
[Posterior ischaemic optic neuropathy]
[Here one case report of the posterior ischaemic optic neuropathy, a rare and underdiagnosed form of the non arteritic ischaemic optic neuropathy is presented, to underline the value of the MRI in the diagnosis. The ischaemic optic neuropathy is the infarction of the optic nerve. Depending on the affected segment of optic nerve (optic nerve head or retrobulbar segment) two subclasses exist: the anterior (AION) and the posterior (PION) ischaemic optic neuropathy. Ischaemic optic neuropathy characterized by sudden, painless, mononuclear loss of vision, and/or visual field defect, that is accompanied by a diagnostic picture of the optic disc fundus only in the case of the AION. The diagnosis of the PION is based on a diagnosis of exclusion described by Hayreh in 1981. The macular and retinal laesions, the etiological role of toxic agent, the compression and the inflammation of the optic nerve all have to be excluded. The differential diagnosis between the PION and the retrobulbar neuritis is more difficult. Nowadays, in addition to the case history and the clinical data the diagnosis of the PION could be confirmed with help of VEP (visual evoked potential) and MRI. In the case of an old woman who had a sudden, painless visual loss of left eye we confirmed the diagnosis of PION with MRI which was presumed after had excluding other etiological factors.]
Clinical Neuroscience
JUNE 02, 2009

[Datas and facts to the history of the neuro-psychiatry - Szent István Kórház, Budapest (1885-2008)]
[Datas and facts to the history of the neuro-psychiatry - Szent István Kórház, Budapest (1885-2008) 2009;62(05-06)]
Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

Clinical Neuroscience
JUNE 02, 2009

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.