The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
LAM KID - 2011;1(03)
Content
LAM KID
DECEMBER 23, 2011
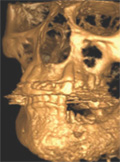
[Osteonecrosis of the jaws: real and unreal scares]
[Osteonecrosis caused by bisphosphonates has been known for a long time, but it is still not widely known. Some people overestimate the danger caused by this disease, whereas others underrate it. In this paper, we summerise data from the international literature and our experiences concerning 93 patients treated at our clinic. We discuss the already known details of the pathomechanism of this disease, its risk factors, the diagnostic methods, the specific stages of the disease and the treatment approaches. Considering the difficulties of treatment, we can't emphasise enough the importance of prevention, since the development of this complication can be minimised even in patients at risk with dental sanation before the bisphosphonate therapy and/or with further intervention performed with antibiotic preventive therapy. We must also point out the importance of early diagnosis and of directing these patients to the appropriate specialist units.]



LAM KID
DECEMBER 23, 2011
[The pathogenic and clinical significance of the RANK-RANKL-osteoprotegerin system in rheumatoid arthritis]
[Rheumatoid arthritis (RA) is characterised by increased local and generalised bone resorption, which manifests in the develoment of marginal erosions and generalised osteoporosis, respectively. An increasing number of data suggest that lymphocytes, proinflammatory cytokines and other mediators involved in inflammation contribute to arthritic bone resorption. Therefore, the term ‘osteoimmunology’ has also become widely used. In RA, Receptor Activator of Nuclear Factor kappa B (RANK) and its ligand (RANKL) play a crucial role in bone resorption. These proteins, which belong to the tumor necrosis factor a (TNF-a) receptor and TNF ligand superfamilies, respectively, activate osteoclasts while interacting with T cells, synovial fibroblasts and other cytokines (e.g. IL-1, IL-17), which results in bone resorption. Osteoprotegerin (OPG) is a decoy receptor that also belongs to the TNF receptor family and inhibits RANK-RANKL interactions. There is increased RANKL production and decreased OPG production in RA. The interaction of RANKL with IL-17 is particularly important. Regarding therapy, sulfasalazine, methotrexate and biological agents, especially TNF inhibitors suppress RANKL-mediated bone resorption and thus the development of joint erosions. RANKL-RANK interaction can be directly inhibited by recombinant OPG or anti-RANKL antibody (denosumab). Among these agents, denosumab gave promising results in experiments performed in animal models of arthritis. These were followed by a phase II human RA trial, which proved that denosumab decreased MRI erosion scores in RA.]
LAM KID
DECEMBER 23, 2011

[Extraskeletal effects of parathyroid hormone]
[The parathyroid gland and its product, parathyroid hormone (PTH) have been subjects of interests in biomedical research for 150 years. Early studies, understandably, concentrated on the primary function: the regulation of serum calcium level. In the past few decades, however, more and more data have shown that, in contrast with the classical view, PTH receptors are expressed not only on bone and kidney cells, but in almost all organs of the human body. Therefore, the effect of PTH obviously cannot be limited to the regulation of bone and mineral metabolism. Systemic symptoms of hyperparathyroidism also became more understandable and explicable by the results of studies on the extraskeletal effects of PTH. Despite the intensive research, the mechanisms of PTH-mediated effects are not well understood in a number of areas. Therefore, it is of great importance to perform further studies in this field, which will hopefully expand our knowledge soon. In our current work, we aim to summarise the nonclassical, extraskeletal effects of PTH (that is, those not related to the regulation of bone metabolism and kidney function) and the results of related studies.]
LAM KID
DECEMBER 23, 2011

[The results of the Ca-Intake.hu study - Calcium supplementation as a part of basic therapy of osteoporosis is more than a routine step]
[Calcium intake is considered the base therapy of osteoporosis treatment. It is known that in case of inadequate calcium intake, specific anti-osteoporotic drugs are inefficient. In the present study, we aimed to investigate the alimentary and supplementary calcium intake among Hungarian osteoporotic patients, using a nationwide representative survey. Patients with osteoporosis were enrolled in the study. We determined the total alimentary calcium intake and the average supplementary dose. In some cases, total calcium intake was lower than recommended, in other cases it was significantly higher than that. In some cases, bone density showed a positive correlation with calcium intake. Vitamin D supplementation complied with current recommendations.]
LAM KID
DECEMBER 23, 2011

LAM KID
DECEMBER 23, 2011

LAM KID
DECEMBER 23, 2011

[The relationship of coronary heart disease and bone from a different point of view: is lumbar vertebral density a positive predictor of coronary heart disease in women?]
[BACKGROUND - A number of international data demonstrate the relationship between cardiovascular disease and bone density, osteoporosis and osteopenia. It is possible that bone formation/remodeling and vascular calcification are influenced by common pathogenetic factors (adipocytokines, inflammatory processes). Our aim was to assess this relationship among Hungarian patients. PATIENTS AND METHODS - We examined 82 patients (49 men and 33 women). The patients underwent a DEXA measurement and fasting blood sampling with full metabolic profiling within one month following an elective coronarography. Coronary state was characterised by the Gensini-score. RESULTS - Femur neck T-score values showed significant decreases in the CHD+ group (patients having at least one significant coronary stenosis), compared with the CHD- group (patients with no history of significant coronary stenosis) (-0.22 vs. -0.85, p<0.05) when the two genders were examined together. In women, lumbar BMD showed a significant positive correlation (r=+0.37, p=0.03), and the levels of adiponectin and HDL-cholesterol showed significant negative correlations (r=-0.311, p=0.04, és r=-0.38, p=0.03) with the Gensini-score. Neither the HOMA-index that characterises insulin resistance, nor the majority of conventional lipid and lipoprotein risk factors showed any association with the severity of coronary heart disease. CONCLUSION - On the basis of our results, the relationships between femur and lumbar regions and coronary heart disease are opposite in nature, which is probably explained by the different regulatory mechanisms in these two regions. Adiponectin may have an important role in the regulation of this relationship, which is independent of insulin resistance.]
LAM KID
DECEMBER 23, 2011

LAM KID
DECEMBER 23, 2011

LAM KID
DECEMBER 23, 2011

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.