The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Hungarian Radiology - 2005;79(04)
Content
Hungarian Radiology
AUGUST 10, 2005




Hungarian Radiology
AUGUST 10, 2005
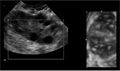
[Ethiopathogenesis of polycystic ovarian syndrome and imaging diagnostics of polycystic ovary]
[Polycystic ovarian syndrome is a heterogenous syndrome with a wide variety of endocrine and metabolic abnormalities and clinical symptoms. It is considered as the most frequent endocrine disorder in women in reproductive age and the most common cause of anovulatory infertility. Key features include menstrual cycle disturbance, hyperandrogenism and obesity. There are many extraovarian aspects to the pathophysiology of polycystic ovarian syndrome, but ovarian dysfunction is central. The underlying unique feature of the ovarian morphology gives the significance of the ultrasound examination. At a recent consensus meeting, a refined definition of the polycystic ovarian syndrome was agreed, encompassing a description of the morphology of the polycystic ovary. The subjective appearance of polycystic ovary should not be substituted for the definition. Further, a woman having polycystic ovary in the absence of menstrual disorder or hyperandrogenism (asymptomatic polycystic ovary) should not be considered as having polycystic ovarian syndrome, until more is known about the situation. Since ultrasound description of polycystic ovary morphology has central role in the diagnosis, and untreated polycystic ovarian syndrome carries long term health risks, the increasing attention to ovarian morphology may offer an effective tool to decrease women`s morbidity. This review outlines the background and feature of ovarian morphology in polycystic ovarian syndrome, and details the current ultrasound definition of polycystic ovary.]
Hungarian Radiology
AUGUST 10, 2005

[Results of non-operative pathological breast diagnostics - One year experience at the Bács-Kiskun County Teaching Hospital]
[INTRODUCTION - Non-operative cytological and histopathological assessment of breast lesions are part of the triple (physical, imaging and pathologic) diagnostic approach and allow a more precise planning of surgical procedures. Both methods have advantages and disadvantages; currently, core biopsy is believed to be more efficient in reaching the diagnostic target. PATIENTS AND METHODS - Breast specimens with a histological diagnosis at the Department of Pathology of the Bács-Kiskun County Teaching Hospital were analysed for their preoperative pathology, using the conventional C1-5 and B1-5 diagnostic categories. RESULTS - 295 cytology and 130 core needle biopsy cases were analysed. The rate of non diagnostic (C1 and B1) material was higher for cytology (0.18 versus 0.08 in general; 0.09 versus 0.01 for malignant cases). The rate of cases with an uncertain diagnostic category (C3 and C4 or B3 and B4) was also higher for the cytology specimens (0.24 versus 0.07). False-negative and false-positive cases were rare, but still more frequent among cytology specimens. CONCLUSION - Core needle biopsy performs better than fine needle aspiration cytology in the establishment of a nonoperative diagnosis at our institution. Despite these results, cytology continues to be the first diagnostic choice, because of its relatively low costs.]
Hungarian Radiology
AUGUST 10, 2005

[Breast core needle biopsies yielding uncertain results - Experience at the complex mammographic screening unit in Kecskemét]
[INTRODUCTION - On occasion core biopsies yield an inconclusive (B3 or B4) result in the triple diagnostics of breast lesions. These cases may turn to be malignant in the operation specimen. This study evaluates the value of B3 and B4 diagnoses and the consequences of these diagnoses. MATERIALS AND METHODS - Core needle biopsies were generally taken under imaging guidance with an automatic gun using G14 gauge needles. They were evaluated using internationally and nationally accepted categories from B1 to B5. The analysis was based on data collected between 2000 and March 2005. RESULTS - Of the 663 core needle biopsy specimens 31 (4.7%) were classified as B3 and 22 (3.3%) as B4. Specimens were more often fragmented in the latter category (a rate of 0.64 as compared with a rate of 0.26). Patients with a B3 diagnosis were operated on in 23 cases, eight of which turned to be malignant (0.35). B4 diagnoses were followed by operations in 21 cases and were found to be malignant on 19 occasions (0.9). Whenever a B4 diagnosis was associated with radiological findings of malignancy (category 5 on mammography and/or ultrasound) the cases unanimously proved to be malignant. The same association with B3 diagnoses yielded malignancy in a rate of only 0.67. CONCLUSION - Both B3 and B4 diagnoses represent an indication for operation. Our experience suggests that B4 diagnoses when coupled with a radiological opinion of malignancy can be candidates for definitive (therapeutic breast conserving) surgery whereas B3 diagnoses require diagnostic excisions.]
Hungarian Radiology
AUGUST 10, 2005

[The glove-finger phenomenon on postero-anterior chest radiograph]
[INTRODUCTION - The glove-finger phenomenon observed on chest plain film is characterized by branching tubular or fingerlike opacities that originate from the hilum and are peripherally directed. This change brings about impaction and inspissation of the mucus and inflammatory debris besides the obstruction of bronchi and of its prestenotic dilatation about. CASE REPORT - A 51 year old male patient presented with coexisting bronchial asthma and microcellular carcinoma of left 2nd pulmonary segment, leading to a tubular type glovefinger phenomenon. The diagnosis was proved by decrease of Tiffeneau’s index, bronchoscopy, bronchocytology and bronchogenic biopsy. CONCLUSION - The glove-finger phenomenon is correctly visible on postero-anterior chest plain film. The dilated and mucus-filled bronchi are not visible on radiography if the sorrounding lung is atelectasic. Because obstructive and nonobstructive bronchogenic diseases can appear with similar presentation, therefore, definitive diagnosis is only possible on the basis of pneumodynamic examinations, bronchoscopy, bronchocytology and biopsy.]
Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

Hungarian Radiology
AUGUST 10, 2005

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
3.
4.
5.