The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Specialities
Gastroenterology
Clinical Neuroscience
MARCH 30, 2024
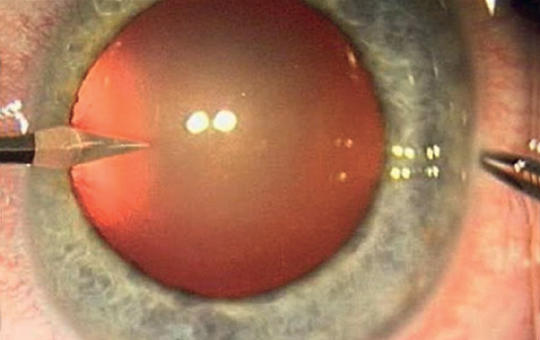
[Thrombolysis treatment and multi- disciplinary management of central retinal artery occlusion in comparison with traditional ophthalmological treatment options ]
[The management of central retinal artery occlusion (CRAO) has long been conservative therapy with limited efficacy carried out in ophthalmology departments together with etiological investigations lacking a standardised protocol. However, CRAO is analogous to ischemic central nervous system stroke and is associated with increased stroke risk, thus, systemic thrombolysis treatment and multidisciplinary management can be beneficial. Since May 2022, at Semmelweis University CRAO patients diagnosed within 4.5 hours are given intravenous thrombolysis therapy and undergo etiologic workup based on current stroke protocols. Here we report our experience with the multidisciplinary, protocol-based management of CRAO in comparison with former non-protocol based ophthalmological conservative treatment.
We reviewed CRAO patients’ data treated conservatively and with paracentesis within 6 hours at the Department of Ophthalmology between 2013 and 2022 including changes in visual acuity, neurological and cardiovascular findings compared to those in the thrombolysis project.
Of the 78 patients receiving non-protocol care, visual improvement was seen in 37% with natural course, 47% with conservative treatment and 47% with paracentesis. Four patients had significant carotid stenosis (2 underwent endarterectomy), 1 carotid dissection, 6 cardioembolism and 1 giant cell arteritis. Of the 4 patients within 4,5 hours, 3 gave their consent to the clinical trial and were treated with thrombolysis and underwent a full etiological assessment.
2 patients had improved visual acuity, 2 patients had significant carotid stenosis and underwent endarterectomy, 1 patient was started on anticoagulation for newly diagnosed atrial fibrillation.
CRAO patients presenting within 4,5 hours are rare and more patients are needed in our study to establish the efficacy of thrombolysis. However uniform protocollized evaluation helps identifying embolic sources thus, avoiding further and potentially more serious thromboembolic events.]



Clinical Neuroscience
MARCH 30, 2024
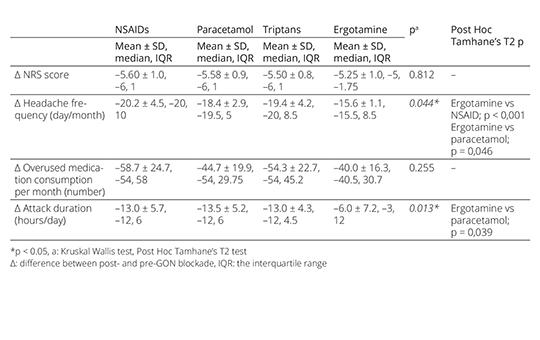
The effect of anesthetic blockade of greater occipital nerve during the withdrawal period of the medication overuse headache treatment
Discontinuation of medication still remains a key element in the treatment of medication overuse headache (MOH), but there is no consensus on the withdrawal procedure. We aimed to share the promising results of anesthetic blockade of greater occipital nerve (GON), which can be an alternative to existing treatments during the early withdrawal period of MOH treatment.
Clinical Neuroscience
MARCH 30, 2024
Perineural 5% dextrose versus corticosteroid injection in non-surgical carpal tunnel syndrom treatment
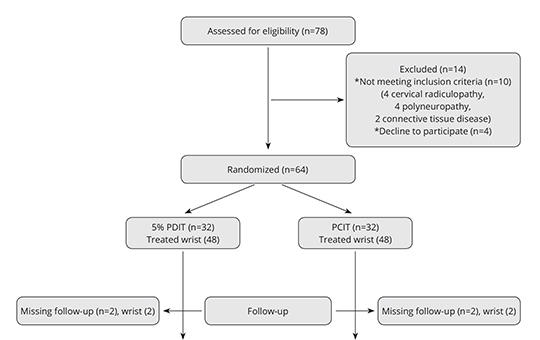
We aimed to investigate the difference of clinical and electrophysiological improvement between perineural corticosteroid injection therapy (PCIT) and perineural 5% dextrose injection therapy (5%PDIT) in carpal tunnel syndrome (CTS).
Total of 92 wrists that were diagnosed as mild-to-moderate idiopathic CTS and completed their follow-up were included in our study. The severity of pain, symptom severity and functional status were assessed by visual analog scale (VAS) and the Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) scores for treatment effectiveness. Randomized wrists were administered PCIT or 5%PDIT accompanied by ultrasound guidance. VAS, BCTQ scores and the electrophysiological study repeated before and after treatment at the 1st and 6th months after perineural injection therapies (PITs) were recorded.
Compared with baseline data, within groups there was significant improvement in VAS, BCTQ severity and function scores at 1st and 6th months follow-up (all p < 0.001). Considerable advance were detected in the median sensory nerve conduction velocity (SNCV) when pretreatment values were compared with posttreatment first month in both groups (p = 0.01; p < 0.001, respectively). No significant change occurred in median distal motor latency (DML) values between the 1st and 6th months in the groups (p = 0.095; p = 0.113, respectively). No significant difference was observed between 5%PDIT and PCIT groups.
Clinical and electrophysiologic improvement in CTS began from 1st month after PCIT and 5%PDIT. At the 6th month follow-up of the patients, 5%PDIT and PCIT had similar therapeutic effects. As a result, we can consider the replacement of PCIT with 5%PDIT in mild-to-moderate CTS patients especially in those who are hesitant because of the corticosteroid’s adverse effects.
Clinical Neuroscience
MARCH 30, 2024
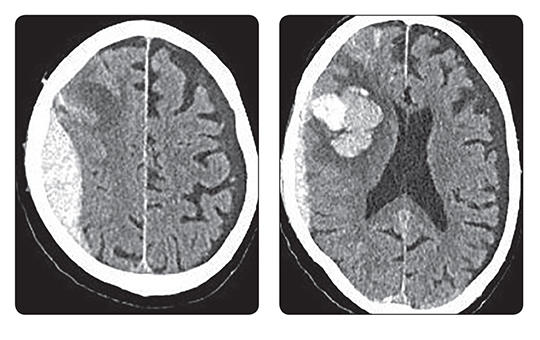
[Middle meningeal artery embolization to treat acute epidural haematoma, case report and literature review ]
[The treatment of acute epidural haematoma is surgery as soon as possible, elimination of the source of bleeding and evacuation of the haematoma. In case of small epidural haematoma, strict neurological and radiological follow-up is necessary. In a significant percentage of cases, open surgery must also be performed within a few days. In case of small epidural haematomas, embolization of the middle meningeal artery is considered as an alternative solution. We review the literature on middle meningeal artery embolization and present our first treatment. Our case report is the first European report about an acute epidural haematoma which was treated by embolization of middle meningeal artery. Our case study is the first report in which a patient was treated with both open surgery and endovascular treatment for acute epidural haematoma within a year.]
Lege Artis Medicinae
MARCH 26, 2024

[Reducing the risk of atrial fibrillation]
[Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia that can lead to thromboembolic events, including cerebral vascular catastrophe and peripheral embolization. AF treatment while managing directly the arrhythmia aims anticoagulation therapy and prevention of thromboembolic events too.
This study overviews the factors influencing the risk of bleeding while managing AF, and focuses especially on appropriate anticoagulant choice, its tailored use to patient characteristics, management of comorbidities and strategies of reducing risks of bleeding.
This analysis compares the efficacy and safety of specific anticoagulants (VKA, DOAC) while considering the patient characteristics such as renal function and comorbidities in anticoagulation treatment.
The risk of bleeding can be reduced by appropriate anticoagulant choice and its patient-specific administration. Consideration of comorbidities is a key issue to ensure safe and effective treatment. VKA requires maintenance of stable INR values, while DOACs lead to fewer major bleeding events. For planned and emergency interventions, the use of bleeding risk reduction strategies is also important. Consideration of patient characteristics, such as renal function and comorbidities, as well as appropriate anticoagulant choice and use are essential to ensure efficient and safe anticoagulation therapy.
]
Clinical Neuroscience
JANUARY 30, 2024
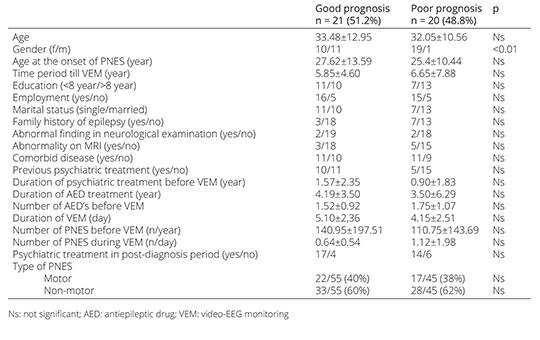
Factors affecting long-term prognosis in adult patients with psychogenic non-epileptic seizures
Among epileptic patients who are monitored using the video-electroencephalography monitoring (VEM) technique, in some patients a psychogenic non-epileptic seizure (PNES) can be identified as a definitive diagnosis. The longterm prognosis of these patients is not well known. In this study, we aimed to determine the factors that affect the prognosis of PNES. Forty-one PNES patients diagnosed using VEM between 2012 and 2022
1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.