The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
LAM KID - 2013;3(03)
Content
LAM KID
OCTOBER 04, 2013

[Vitamin D treatment: hormone therapy for patients who need it or simply a supplementation for everyone?]
[Various medical associations issue different recommendations for the prevention and treatment of vitamin D deficiency. These significant differences are partly explained by the different definition of normal vitamin D level and the use of completely different mathematical models to predict the increase in vitamin D level as a response to therapy. According to the Institute of Medicine (IOM), the target vitamin D level is 20 ng/ml, whereas the Endocrine Society (ES) recommends 30 ng/m as the miminum target value. According to the ES, a 1 ng/ml increase of vitamin D level can be reached by a daily intake of 100 NE, while the IOM recommends 3.6 ng/ml. Moreover, the IOM states that the effect of therapy on serum level is nonlinear. These differences show that the ES and IOM have different views on the risk of adverse effects. The IOM recommends 400 IU vitamin D daily for children younger than 1 year, 800 IU for those above 70 years and 600 IU/per day for everyone else. The ES recommend 400-1000 IU daily for all infants and 1500- 2000 IU for adults. Screening, however, is not recommended by either society. To decrease uncertainty concerning the side effects of higher-dose vitamin D treatment, it is important to understand, use and support the function of the pharmacovigilance system of the pharmaceutical industry that manufactures and markets various (prescription, over-the-counter) preparations. This is what the author aims to highlight in the second part of this article. Using this system, both the doctor and the patient can help support and accept the justification of higher-dose vitamin D therapy.]



LAM KID
OCTOBER 04, 2013

[Is a paradigm shift possible in the clinical practice of preventing recurrent fractures?]
[Recurrent osteoporotic bone fractures are less and less considered “natural”, due to the immense variety of products available for treatment. In order to prevent recurrent fractures, treatment should be started in time, and a careful approach is needed to choose the appropriate treatment, and, if needed, to switch therapy. When choosing the therapeutic approach, we have to decide whether it corresponds to the severity of the osteoporosis and the risk of fracture. In order to do this, we have to consider bone quality, previous fractures, the condition of cortical bones and the mode of action of the selected treatment, in addition to the easily evaluated density value. The aim of this article is to provide practical help for the above mentioned decisionmaking process.]
LAM KID
OCTOBER 04, 2013

[A simple method to detect urate crystals in formalin-fixed tissue]
[In our previous study we refuted the thesis that sodium urate crystals are not, or only rarely detectable in formalin-fixed histological samples because they dissolve in the aqueous formalin solution. Our observations indicate that dissolution of urate crystals is primarily caused by haematoxylineosin staining. Undeniably, however, urate crystals are partially dissolved in the aqueous solution of formaldehyde, and thus a small amount of urate deposits may totally dissolve from tissue samples. The aim of the present study was to identify those steps of the staining procedure that are responsible for the dissolution of urate crystals. We found that the dissolution of urate crystals during the course of staining was caused by the combined effects of haematoxylin staining, treatment with 1% aqueous lithium carbonate solution and dehydration with acetone. As the simplest histological method for the detection of urate crystals, we recommend examining unstained sections (mounted with Canada balsam) of formalin-fixed, paraffin-embedded tissue samples in polarised light. According to our previous study, about two thirds of urate crystals remain detectable on unstaied sections, whereas haematoxylin-eosin stained sections of the same tissue samples (derived from patients with gout) did not contain urate crystals. In the samples where urate crystals could be detected in haematoxylin- eosin stained sections using polarised light, the unstained sections contained much more crystals, which shows that dissolution is greatly decreased on unstained sections.]
LAM KID
OCTOBER 04, 2013

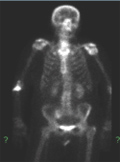
[Sacral insufficiency fractures]
[BACKGROUND - The spontaneous osteoporotic fracture of the sacrum, known as a sacral insufficiency fracture (SIF) was first described as an unrecognized syndrome of the elderly by Laurie, in 1982. Numerous case histories and a few series of cases have been discussed in medical journals; however, none have been reported in Hungary. GOAL - To delineate the leading diagnostic steps in the recognition of SIF and review the therapeutic guidelines. CASE HISTORIES, METHODS - Between January 2009 and the first six months of 2010 11 cases of SIF were diagnosed at the National Center for Spinal Disorders. We examined the clinical aspects of the illness, the radiological modalities, the fracture markings, the pace of recovery and duration. RESULTS - The 11 patients were found to have various SIF predestining etiological factors and the following classic fractures - H-type, unilateral, horizontal, unilateralhorizontal and vertical as well as a bilateral pattern. In cases often not showing obvious clinical symptoms and in cases resulting in conventional radiological examinations of low sensitivity and specificity, we used mapping techniques in setting up the exact diagnosis. CONCLUSION - If we consider SIF from patient history and known risk factors, diagnostic procedure (primer original) may be shortened and a number of unnecessary tests (biopsy) may be avoided.]
LAM KID
OCTOBER 04, 2013
[Infective sacroiliitis]
[INTRODUCTION - Pyogen infection of the sacroiliac joint occurs rarely in rheumatological practice. Its clinical symptoms are diverse, so the diagnosis is often made late. CASE REPORT - The author presents a case of a 67-year-old woman. The patient did not have any major diseases nor any predisposing factors for infection. Five days after doing hard physical work she felt strong pain irradiating from her lower back to the right lower limb. She was referred to the Department of Neurology with the diagnosis of right lumbar radiculopathy. She was primarily examined for tumours because of her high red blood cell sedimentation rate and CRP level and her inability to walk. The correct diagnosis was set up on the basis of MRI examination: infective sacroiliitis on the right side, which has spreaded to the adjacent tissues. USguided biopsy was unsuccesful, so empiric antibioitic treatment was started. The patient was discharged from hopsital after 35 days and continued clindamycin therapy at home. At control examination 6 month later she did not have any symptoms or complaints and laboratory examinations did not indicate inflammatory activity. MRI examination still showed an extensive oedema. CONCLUSION - Pyogen arthritis should be considered even in the absence of fever, leukocytosis and predisposing factors. By making the correct diagnosis and starting long-term antibiotic therapy in time, joint destruction is preventable and the patient is curable.]
LAM KID
OCTOBER 04, 2013

LAM KID
OCTOBER 04, 2013

LAM KID
OCTOBER 04, 2013

LAM KID
OCTOBER 04, 2013

LAM KID
OCTOBER 04, 2013

LAM KID
OCTOBER 04, 2013


1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.