The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Hungarian Immunology - 2004;3(02)
Content
Hungarian Immunology
FEBRUARY 15, 2004

[Toll-like receptors and epithelial cells]
[Toll-like receptors have been extensively studied in the last few years. These receptors are involved in the mechanisms how microbes and infections are linked to natural immunity and some autoimmune-inflammatory processes. Here author reviews the latest news on Tolllike receptors with much emphasis on their role on epithelial cells. Therapeutic strategies targeting Toll-like receptors are also discussed.]



Hungarian Immunology
FEBRUARY 15, 2004

[Experiences on cyclosporin-A treated childhood atopic dermatitis resistant to other therapies]
[BACKGROUND - Cases of six children suffering from serious form (resistant to conventional therapy) of atopic dermatitis are presented and the experiences regard of treatment with cyclosporin A (Sandimmun Neoral-microemulsion form) are summarised. PATIENTS - The average age of the 4-16 year-old children (three girls, three boys) was 9.9 years. The skin process started at infantile age. The cyclosporin A was used during 12-85 weeks, in a maximal dose of 3.5-5 mg/body weight kg/day. The patients received locally creams or ointments to moisture their skin continuously and if it was necessary, corticosteroid creams or ointments for a few days. RESULTS - The therapeutic response was excellent in five cases and poor in one case. The short time therapies resulted transient, the long time therapies long acting effect. There was no side effect indicating the stop of cyclosporin A therapy. Three children presented body weight elevation slightly higher than the age-related physiologic change. Epstein-Barr and cytomegalovirus infection with severe submandibular lymphadenopathy appeared in a patient and transient hypertrichosis in the case treated for 85 weeks. DISCUSSION - The authors propose treating severe childhood atopic dermatitis resistent to other therapeutic possibilities with cyclosporin A. The adequate follow up, monitoring of clinical and bloodchemical parameters are important.]
Hungarian Immunology
FEBRUARY 15, 2004

[SS-A(Ro) and SS-B(La) autoantibodies in systemic lupus erythematosus]
[OBJECTIVE - To assess the relation between clinical features and the presence of SS-A(Ro) and SS-B(La) autoantibodies in systemic lupus erythematosus. PATIENTS - The data of 200 patients with definite systemic lupus erythematosus were analysed. SSA( Ro) and SS-B(La) antibodies were assessed by enzyme immunoassay. RESULTS - 40.5% of systemic lupus erythematosus' patients were SS-A(Ro) and/or SS-B(La) antibody positive (’positive group’); the majority of such patients displayed both antibodies, 16.5% had SSA( Ro) antibodies alone, while only 2% has SS-B(La) antibodies alone. There were no differences in the occurrence of arthritis, secondary antiphospholipid syndrome and hematologic manifestations between the positive and negative groups; serositis was more common in the positive group. Skin manifestations, in particular subacute cutaneous lupus erythematosus and urticaria vasculitis were more frequent in the positive group, while kidney and central nervous system involvation, in particular severe forms were less frequent. Secondary Sjögren's syndrome occurred exclusively in antibody positive patients. Sm, RNP and Scl-70 antibodies were more frequently found in the positive group. CONCLUSIONS - The presence of SS-A(Ro) and/or SS-B(La) antibodies in systemic lupus erythematosus has some prognostic significance; in antibody-positive patients there is an increased risk for skin lesions (in particular subacute cutaneous lupus erythematosus and urticaria vasculitis) and secondary Sjögren’s syndrome and a decreased risk for severe nephritis or central nervous system involvement.]
Hungarian Immunology
FEBRUARY 15, 2004

[β-endorphin concentrations in the cerebrospinal fluid and serum in systemic lupus erythematosus and multiple sclerosis patients]
[INTRODUCTION - The aim of the present study was to investigate the cerebrospinal fluid and serum β- endorphin levels in several diseases characterized by central nervous system demyelinisation. PATIENTS AND METHODS - Ten patients with systemic lupus erythematosus complicated with demyelinating syndrome and ten patients with chronic progressive form of multiple sclerosis were selected. Concentrations of β-endorphin were measured using a high sensitive, specific radioimmunoassay. Statistical significance (Wilcoxon test, two variable t test) and correlations (Spearman and Pearson correlations coefficients) were calculated. RESULTS - β-endorphin concentration in the cerebrospinal fluid did not differ in multiple sclerosis and systemic lupus erythematosus patients compared to the controls.]
Hungarian Immunology
FEBRUARY 15, 2004

Hungarian Immunology
FEBRUARY 15, 2004
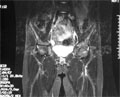
[Diagnostic value of MRI in patients with juvenile dermatomyositis]
[Diagnosis of juvenile dermatomyositis is based on the presence of proximal muscle weakness, characteristic skin lesions, muscle enzyme elevation in the serum, and may requires the performance of invasive procedures such as electromyography and/or muscle biopsy. Magnetic resonance imaging (MRI) is considered to be an objective non-invasive tool to detect muscle involvement for diagnosis as well as for follow-up studies. We report a case of a 12 years old girl with definitive juvenile dermatomyositis. She received glucocorticoid therapy and achieved remission of the disease. After a long-term relapse free period, she was presented with severe proximal muscle weakness and normal creatinine kinase levels. The laboratory studies did not reveal acute inflammation or infection. In this case MRI was diagnostic to the relapse of juvenile dermatomyositis, with an increased STIR (short tau inversion recovery) signal of proximal muscles. The muscle involvement detected by MRI correlated with functional ability. After she achieved clinical remission, further follow-up MRI scans demonstrated that the affected muscles had returned to normal signal intensity. Findings of dermatomyositis on MRI scans include increased signal intensity in the affected muscles, perimuscular edema, chemical-shift artifact, and increased signal intensity in subcutaneous tissue. MRI is a sensitive technique and proposed to be a good indicator for an early diagnosis of the disease. MRI may also help to guide the muscle biopsy and may enhance the sensitivity of histological examination. After completion of therapy, MRI may be used for monitoring the progress of the disease as signal intensity of affected muscles returns to normal. MRI is also helpful, if the diagnosis is suspected but has not been formally evaluated.]
Hungarian Immunology
FEBRUARY 15, 2004

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
3.
4.
5.