The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2020;73(05-06)
Content
Clinical Neuroscience
MAY 30, 2020
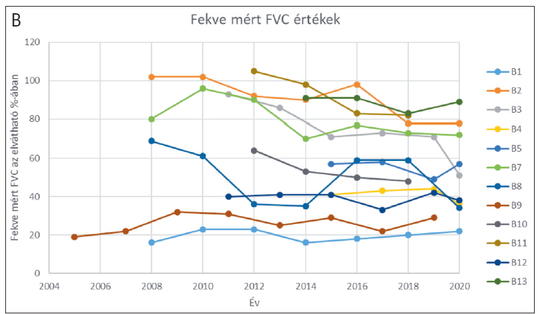
[The long-term follow-up of enzyme replacement treatment in late onset Pompe disease]
[Pompe disease (PD) is a rare lysosomal disease caused by the deficient activity of acid alpha-glucosidase (GAA) enzyme due to mutations in the GAA gene. The enzymatic deficiency leads to the accumulation of glycogen within the lysosomes. Clinically, the disease has been classically classified in infantile and childhood/adult forms. Presently cc. close to 600 mutations distributed throughout the whole gene have been reported. The c.-32-13T>G splice mutation that is very common in patients of Caucasian origin affected by the childhood/adult form of the disease, with an allelic frequency close to 70%. Enzyme replacement treatment (ERT) is available for the patients with Pompe disease (Myozyme). In this paper, we are presenting the long term follow up of 13 adult onset cases treated more than 5 years. The longest follow up was 15 years. To evaluate the treatment efficacy, the 6 minutes walking test (6MWT) and the respiratory functions were monitored annually. The analysis revealed that at the beginning of ERT for 3-4 years the 6MWT had been generally increasing, then it declined, and after 10 years it was lower in 77% of the cases than it had been at the start of the treatment. In 23% of the cases the 6MWT increased during the follow up time. Only one of the patients become wheelchair dependent during the follow-up period. The respiratory function showed similar results especially in supine position. A high degree of variability was observed among patients in their responses to the treatment, which only partially associated with the antibody titer against the therapeutic protein. The efficacy of the ERT was associated with the type of the disease causing mutation, the baseline status of the disease, the lifestyle and the diet of the patient. The long-term follow up of the patients with innovative orphan drugs is necessary to really understand the value of the treatment and the need of the patients.]



Clinical Neuroscience
MAY 30, 2020

[Family planning in multiple sclerosis: conception, pregnancy, breastfeeding]
[Family planning is an exceptionally important question in multiple sclerosis, as women of childbearing age are the ones most often affected. Although it is proven that pregnancy does not worsen the long-term prognosis of relapsing-remitting multiple sclerosis, many patients are still doubtful about having children. This question is further complicated by the fact that patients – and often even doctors – are not sufficiently informed about how the ever-increasing number of available disease-modifying treatments affect pregnancies. Breastfeeding is an even less clear topic. Patients usually look to their neurologists first for answers concerning these matters. It falls to the neurologist to rationally evaluate the risks and benefits of contraception, pregnancy, assisted reproduction, childbirth, breastfeeding and disease modifying treatments, to inform patients about these, and then together come to a decision about the best possible therapeutic approach, taking the patients’ individual family plans into consideration. Here we present a review of relevant literature adhering to international guidelines on the topics of conception, pregnancy and breastfeeding, with a special focus on the applicability of approved disease modifying treatments during pregnancy and breastfeeding. The goal of this article is to provide clinicians involved in the care of MS patients with up-to-date information that they can utilize in their day-to-day clinical practice. ]
Clinical Neuroscience
MAY 30, 2020
[Neurological aspects of the COVID-19 pandemic caused by the SARS-CoV-2 coronavirus]
[By the spring of 2020 the COVID-19 outbreak caused by the new SARS-CoV-2 coronavirus has become a pandemic, requiring fast and efficient reaction from societies and health care systems all over the world. Fever, coughing and dyspnea are considered the major signs of COVID-19. In addition to the involvement of the respiratory system, the infection may result in other symptoms and signs as well. Based on reports to date, neurological signs or symptoms appear in 30-50% of hospitalized COVID-19 patients, with higher incidence in those with more severe disease. Classical acute neurological syndromes have also been reported to associate with COVID-19. A drop in the volume of services for other acute diseases has been described in countries with healthcare systems focusing on COVID-19. During the COVID-19 epidemic it is also important to provide appropriate continuous care for those with chronic neurological disorders. It will be the task of the future to estimate the collateral damage caused by the COVID-19 epidemic on the outcome of other neurological disorders, and to screen for the possible late neurological complications of the SARS-CoV-2 coronavirus infection.]
Clinical Neuroscience
MAY 30, 2020

Creutzfeldt-Jakob Disease: A single center experience and systemic analysis of cases in Turkey
We aimed to analyze the clinical, laboratory and neuroimaging findings in patients with sporadic Creutzfeldt-Jakob disease (CJD) in a single center as well as to review other published cases in Turkey. Between January 1st, 2014 and June 31st, 2017, all CJD cases were evaluated based on clinical findings, differential diagnosis, the previous misdiagnosis, electroencephalography (EEG), cerebrospinal fluid and cranial magnetic resonance imaging (MRI) findings in our center. All published cases in Turkey between 2005-2018 were also reviewed. In a total of 13 patients, progressive cognitive decline was the most common presenting symptom. Two patients had a diagnosis of Heidenhain variant, 1 patient had a diagnosis of Oppenheimer-Brownell variant. Seven patients (53.3%) had been misdiagnosed with depression, vascular dementia, normal pressure hydrocephalus or encephalitis. Eleven patients (87%) had typical MRI findings but only 5 of these were present at baseline. Asymmetrical high signal abnormalities on MRI were observed in 4 patients. Five patients (45.4%) had periodic spike wave complexes on EEG, all appeared during the follow-up. There were 74 published cases in Turkey between 2005 and 2018, with various clinical presentations. CJD has a variety of clinical features in our patient series as well as in cases reported in Turkey. Although progressive cognitive decline is the most common presenting symptom, unusual manifestations in early stages of the disease might cause misdiagnosis. Variant forms should be kept in mind in patients with isolated visual or cerebellar symptoms. MRI and EEG should be repeated during follow-up period if the clinical suspicion still exists.
Clinical Neuroscience
MAY 30, 2020
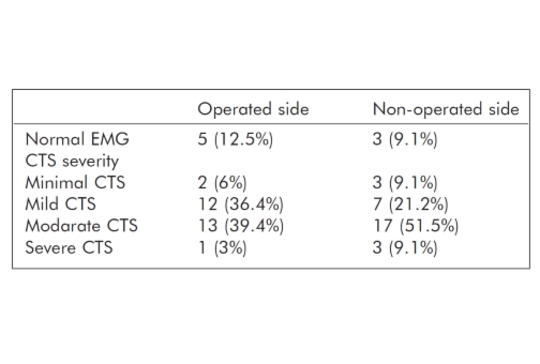
Autonomic nervous system may be affected after carpal tunnel syndrome surgery: A possible mechanism for persistence of symptoms after surgery
After carpal tunnel surgery, some patients report complaints such as edema, pain, and numbness. Purpose – The aim of this study was to evaluate autonomic nervous system function in patients with a history of carpal tunnel surgery using sympathetic skin response (SSR). Thirty three patients (55 ±10 years old) with a history of unilateral operation for carpal tunnel syndrome were included in the study. The SSR test was performed for both hands. Both upper extremities median and ulnar nerve conduction results were recorded. A reduced amplitude (p=0.006) and delayed latency (p<0.0001) were detected in the SSR test on the operated side compared to contralateral side. There was no correlation between SSR and carpal tunnel syndrome severity. Although complex regional pain syndrome does not develop in patients after carpal tunnel surgery, some of the complaints may be caused by effects on the autonomic nervous system.
Clinical Neuroscience
MAY 30, 2020
The etiology and age-related properties of patients with delirium in coronary intensive care unit and its effects on inhospital and follow up prognosis
Delirium is a syndrome frequently encountered in intensive care and associated with a poor prognosis. Intensive care delirium is mostly based on general and palliative intensive care data in the literature. In this study, we aimed to investigate the incidence of delirium in coronary intensive care unit (CICU), related factors, its relationship with inhospital and follow up prognosis, incidence of age-related delirium and its effect on outcomes. This study was conducted with patients hospitalized in CICU of a tertiary university hospital between 01 August 2017 and 01 August 2018. Files of all patients were examined in details, and demographic, clinic and laboratory parameters were recorded. Patients confirmed with psychiatry consultation were included in the groups of patients who developed delirium. Patients were divided into groups with and without delirium developed, and baseline features, inhospital and follow up prognoses were investigated. In addition, patients were divided into four groups as <65 years old, 65-75 yo, 75-84 yo and> 85 yo, and the incidence of delirium, related factors and prognoses were compared among these groups. A total of 1108 patients (mean age: 64.4 ± 13.9 years; 66% men) who were followed in the intensive care unit with variable indications were included in the study. Of all patients 11.1% developed delirium in the CICU. Patients who developed delirium were older, comorbidities were more frequent, and these patients showed increased inflammation findings, and significant increase in inhospital mortality compared to those who did not develop delirium (p<0.05). At median 9-month follow up period, rehospitalization, reinfarction, cognitive dysfunction, initiation of psychiatric therapy and mortality were significantly higher in the delirium group (p<0.05). When patients who developed delirium were divided into four groups by age and analyzed, incidence of delirium and mortality rate in delirium group were significantly increased by age (p<0.05). Development of delirium in coronary intensive care unit is associated with increased inhospital and follow up morbidity and mortality. Delirium is more commonly seen in geriatric patients and those with comorbidity, and is associated with a poorer prognosis. High-risk patients should be more carefully monitored for the risk of delirium.
Clinical Neuroscience
MAY 30, 2020
Alexithymia is associated with cognitive impairment in patients with Parkinson’s disease
Cognitive dysfunction (CD) is a common non-motor symptom of Parkinson’s disease (PD). Alexithymia is a still poorly understood neuropsychiatric feature of PD. Cognitive impairment (especially visuospatial dysfunction and executive dysfunction) and alexithymia share common pathology of neuroanatomical structures. We hypothesized that there must be a correlation between CD and alexithymia levels considering this relationship of neuroanatomy. Objective – The aim of this study was to evaluate the association between alexithymia and neurocognitive function in patients with PD. Thirty-five patients with PD were included in this study. The Toronto Alexithymia Scale–20 (TAS-20), Geriatric Depression Inventory (GDI) and a detailed neuropsychological evaluation were performed. Higher TAS-20 scores were negatively correlated with Wechsler Adult Intelligence Scale (WAIS) similarities test score (r =-0.71, p value 0.02), clock drawing test (CDT) scores (r=-0.72, p=0.02) and verbal fluency (VF) (r=-0.77, p<0.01). Difficulty identifying feelings subscale score was negatively correlated with CDT scores (r=-0.74, p=0.02), VF scores (r=-0.66, p=0.04), visual memory immediate recall (r=-0.74, p=0.01). VF scores were also correlated with difficulty describing feelings (DDF) scores (r=-0.66, p=0.04). There was a reverse relationship between WAIS similarities and DDF scores (r=-0.70, p=0.02), and externally oriented-thinking (r=-0.77,p<0.01). Executive function Z score was correlated with the mean TAS-20 score (r=-62, p=0.03) and DDF subscale score (r=-0.70, p=0.01) Alexithymia was found to be associated with poorer performance on visuospatial and executive function test results. We also found that alexithymia was significantly correlated with depressive symptoms. Presence of alexithymia should therefore warn the clinicians for co-existing CD.

Clinical Neuroscience
MAY 30, 2020

[Early experiences in surgical treatment of thoracic disc herniation from posterior transdural approach at Neurosurgery Clinic Szeged University]
[Background – Because of the rare occurrence of thoracic disc herniation and surgery needed treatment the used approaches and their efficiency are still subjects of discussions. In Hungarian practice, the most frequent explorations are costotransversectomy and laminectomy, but there are many other important methods available like thoracoscopic and posterior transdural approaches. This case report will present the benefits and the surgical procedure of posterior transdural sequesterectomy, carry out for the first time in Hungary at the Neurosurgical Department on Szeged University. Case presentation – A 50-year-old female patient with achondroplasic nanism has been operated several times since 2011. She suffered from a progressive, multi-segment affected degenerative discopathy and myelopathy. Finally in the background of the recurrent paraparesis was confirmed thoracic disc herniations at the levels of T8 and T9. The use of intraoperative electrophysiology was not feasable, because the earlier described cervical myelopathy. For this reason we used the posterior transdural approach, as the best and safest, visual control warranted technique. Conclusions – The posterior transdural approach offers an alternative option for experienced surgeons, furthermore in contrast with traditional, technically difficult to implement or special instrumentation demanding approaches this technique seems to be more efficient.]
Clinical Neuroscience
MAY 30, 2020
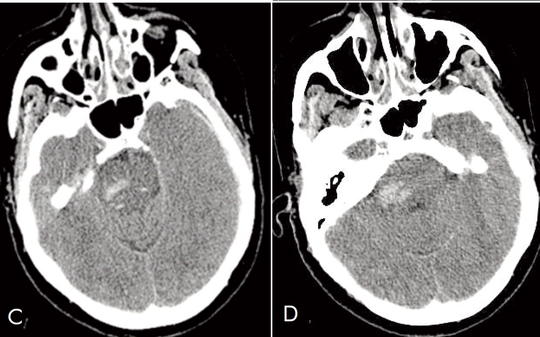
Simultaneous subdural, subarachnoideal and intracerebral haemorrhage after rupture of a peripheral middle cerebral artery aneurysm
The cause of intracerebral, subarachnoid and subdural haemorrhage is different, and the simultaneous appearance in the same case is extremely rare. We describe the case of a patient with a ruptured aneurysm on the distal segment of the middle cerebral artery, with a concomitant subdural and intracerebral haemorrhage, and a subsequent secondary brainstem (Duret) haemorrhage. The 59-year-old woman had hypertension and diabetes in her medical history. She experienced anomic aphasia and left-sided headache starting one day before admission. She had no trauma. A few minutes after admission she suddenly became comatose, her breathing became superficial. Non-contrast CT revealed left sided fronto-parietal subdural and subarachnoid and intracerebral haemorrhage, and bleeding was also observed in the right pontine region. The patient had leucocytosis and hyperglycemia but normal hemostasis. After the subdural haemorrhage had been evacuated, the patient was transferred to intensive care unit. Sepsis developed. Echocardiography did not detect endocarditis. Neurological status, vigilance gradually improved. The rehabilitation process was interrupted by epileptic status. Control CT and CT angiography proved an aneurysm in the peripheral part of the left middle cerebral artery, which was later clipped. Histological examination excluded mycotic etiology of the aneurysm and “normal aneurysm wall” was described. The brain stem haemorrhage – Duret bleeding – was presumably caused by a sudden increase in intracranial pressure due to the supratentorial space occupying process and consequential trans-tentorial herniation. This case is a rarity, as the patient not only survived, but lives an active life with some residual symptoms.
1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.