The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2015;68(01-02)
Content
Clinical Neuroscience
JANUARY 30, 2015




Clinical Neuroscience
JANUARY 30, 2015

[Extending therapeutic possibilities in relapsing-remitting multiple sclerosis: dimethyl fumarate]
[Dimethyl fumarate (DMF) is a novel oral therapy that has recently been approved for the treatment of relapsing- remitting multiple sclerosis (RRMS). Dimethyl fumarate shows anti-inflammatory and cytoprotective properties that are thought to be mediated primarily via activation of the nuclear factor (erythroid-derived 2)-like 2 - Nrf2 transcriptional pathway, which up-regulates the genes involved in the cellular response to oxidative stress. The drug was evaluated in 2 large, randomized, double-blind, multicentric, multinational, 2-year, phase III clinical trials. The DEFINE and CONFIRM trials, conducted with over 2600 adult patients suffering from RRMS, unequivocally confirmed the efficacy of DMF (2×240 mg daily) in reducing the annualized relapse rate (ARR) and reducing the proportion of patients with MS relapse at 2 years. Significantly reduced sustained disability progression was observed with the drug versus placebo in DEFINE, while the same tendency was seen in CONFIRM. The MRI results of the studies were also convincing: DMF significantly reduced the number of new/enlarging T2-hyperintense lesions and the number of Gd-enhancing lesions compared to placebo. Dimethyl fumarate was generally well tolerated and no safety concern has been raised. Adverse events that occurred most frequently included flushing and gastrointestinal events. The long- term efficacy and tolerability of dimethyl fumarate is currently being investigated in the ENDORSE trial, with interim results demonstrating the same results as the two previous studies. In conclusion, although further, mostly comparative data are needed to fully establish the relative efficacy and tolerability of dimethyl fumarate compared with other therapies, dimethyl-fumarate is a valuable addition to the therapeutic options available for RRMS.]
Clinical Neuroscience
JANUARY 30, 2015

[Role of modified open-door laminoplasty in the treatment of multilevel cervical spinal stenosis: a retrospective analysis of 43 cases]
[Background and purpose - Symptomatic degenerative multilevel cervical spinal stenosis - beside other methods - is often treated using the open-door laminoplasty. This procedure aims to decompress the spinal cord and preserve the stability of the cervical spine. The efficiency and safety of the method was proved by numerous Japanese and American studies, also the technique related complications are well known. We treated 43 patients with symptomatic multilevel cervical spine stenosis using the open-door laminoplasty as a surgical procedure of choice in the National Institute of Clinical Neurosciences between 2009 and 2012. In this article we analyse our results and the related literature is discussed. Methods - Symptomatic patients with a minimum of three-segment cervical spine stenosis and radiologically proved myelopathy or with electrophisiologically verified subclinical myelopathy were selected for laminoplasty. Patients in whom cervical kyphosis was present were operated on using laminectomy and posterior fusion. Postoperative control CT, MRI and/or X-ray images were made after the surgery and at six weeks, three, six and 12 months after the operation and in the same time neurological evaluation was performed. The modified Japanase Orthopaedic Association (mJOA) scale value was assigned to patients preoperatively, six weeks, three, six and 12 months after the operation. The statistical difference between the groups of data was tested by chi square test. Results - The average follow-up time was 27 months (minimum seven, maximum 42). According to the mJOA scale, 26 patient’s condition (61%) improved, in 13 cases (30%) remained unchanged, and in one case (2%) we detected neurological deterioration. We lost three patients during the follow up period. The median of mJOA preoperatively was 12 (minimum eight, maximum 18), while six week postoperative mJOA was 14 (minimum 10, maximum 17). Three, six and 12 months mean value of mJOA was 14 which shows that the improvement in patients’ condition remained stable at one year after surgery. The difference was statistically significant (p<0.05). The canal’s average anteroposterior diameter on CT was 8.29±0.92 mm at the level of C III, while after the operation we measured 15.16±1.02 mm; 7.54±0.62 mm at the level of C IV before, and 15.29±0.2 mm after; 9.05±0.48 mm at the level of C V before and 17.23±0.4 mm after the surgery. The differences proved to be significant (p=0.0001). Conclusion - According to our experiences the modified open-door laminoplasty is an efficient and safe method for the treatment of symptomatic multilevel cervical spinal stenosis.]
Clinical Neuroscience
JANUARY 30, 2015

[The efficacy of lacosamide in relation to antiepileptic drug history. Clinical experiences in adult partial epilepsy]
[Objective - A retrospective study in adult partial epilepsy on the efficacy of lacosamide in relation to previous antiepileptic drug experiences. Method - We analysed 3-65 months’ data on epilepsy-care of 43 pharmacoresistant partial epilepsy patients treated with lacosamide. Further analysis of antiepileptic drug history was carried out in strictly selected subgroups of patients with good and poor therapeutic response to lacosamide (10 and 9 patients, respectively) for 2-10 years long retrospective follow up. Patients - Adult patients with partial-onset seizures had been treated previously with three or more lifetime antiepileptic drugs without permanent success. Results - Six patients (14%) were seizure free, eleven patients (25%) have experienced important improvement (their seizure-frequency decreased by at least 50%) for more than 12 months. Fourteen patients (32%) improved for less than 6 months and then have relapsed; and add-on lacosamide proved ineffective in 12 patients (28%). Those selected 10 patients successfully treated with lacosamide (seizure free for at least six months) favourably responded to carbamazepine or oxcarbazepine earlier and levetiracetam was ineffective or even caused worsening. The selected lacosamide-unresponsive nine patients responded unfavourably to carbamazepine or oxcarbazepine earlier. Fifteen patients (35%) suffered side effects as dizziness or sleepiness, in 11 of them lacosamide was combined with a „traditional” sodium-channal blocker antiepileptic drug. Conclusion - Lacosamide is an effective add-on antiepileptic drug in difficult-to treat adult partial epilepsy patients. Our data suggest that good lacosamide response may be expected in those patients who reacted favourably to „traditional” sodium-channel blocker carabamazepine or oxcarbazepine earlier.]
Clinical Neuroscience
JANUARY 30, 2015

[Assessment of severity and time course of critical illness neuropathy in septic patients: a prospective observational study]
[Objective - In this prospective observational study we investigated electrophysiological alterations in the early phase of critical illness and correlated electrophysiological findings with the clinical picture and outcome. Methods - We enrolled 21 critically ill surgical patients having ≥12 Acute Physiology and Chronic Health Evaluation (APACHE) II scores on admission. Routine non-invasive bilateral electroneurography (ENG) examination of median and ulnar nerves was done on five consecutive days starting in two days after admission. Then weekly follow-up was performed. Motor and sensory nerve conduction indices were calculated and correlated with APACHE II and Simplified Acute Physiology Score II severity scores. Results - On the first examination 18/21 patients had >20% reduction in the motor and sensory nerve conduction indices. Severity score systems showed significant negative correlation with the daily change of CMAP and SNAP amplitudes and calculated nerve conduction indices (Spearman’s correlation, p<0,001). Mortality was higher in the patients with worse admission ENG and/or stagnant electrophysiological status or declining tendency in the first week. Conclusions - Electrophysiological alterations appeared soon after the development of critical illness. Early phase alterations showed a strong correlation with patients’ general condition and more severe electrophysiological alterations predisposed to higher mortality. In several cases early alterations proved to be reversible. ]
Clinical Neuroscience
JANUARY 30, 2015

[Intraoperativ electrophysiological monitoring during neurosurgery on eloquent structures]
[Objective - We summarize our experiences on intraoperative electrophysiological monitoring during neurosurgical procedures on eloquent neuronal structures. Patients, methods - Sixty patients were enrolled retrospectively in our study with pathologies involving eloquent neuronal structures. They were operated between May 2011. and March 2012. at the University of Debrecen, Department of Neurosurgery and at the National Institute of Neurosciences. Patients underwent standard preoperative examinations due to the primary pathology. In all cases we used intraoperative electrophysiological monitoring. We had 22 cases with cranial nerve monitoring, 10 cases with cauda monitoring, 16 cases with motor system monitoring, six cases with complex spinal cord monitoring, three degenerative spine reconstructions and 3 awake surgeries. Results - We found that with the use of intraoperative electrophysiology we could make these neurosurgical procedures safer, and were able to optimize the extent of resection in the cases of oncological pathologies. Conclusions - Our experiences as well as the international literature suggests that in certain high risk neurosurgical procedures intraoperative electrophysiology is indispensible for safe and optimally extended operation.]
Clinical Neuroscience
JANUARY 30, 2015

[Efficacy of anticoagulation with vitamin K antagonists in acut stroke patients with atrial fibrillation - Hungarian results]
[Background and objective - An estimated 20% of ischemic strokes are of cardiogenic origin, half of which is associated with atrial fibrillation (AF). Anticoagulation treatment of patients with this arrhythmia reduces their risk of stroke. Effectiveness and safety of oral anticoagulant therapy with vitamin K antagonists (VKA) is limited, however, by their well-known narrow therapeutic window and the substantial inter- and intraindividual variability of INR values depending on genetic and dietary factors as well as drug interactions. Our objective was to evaluate the prevalence of adequate anticoagulation and the level of anticoagulant effect actually achieved among patients with AF hospitalized for acute stroke. Methods - Patients with AF admitted to our hospital ward in 2012 for acute stroke (n=226) were included in the analysis. Using descriptive statistics, relevant clinical and therapeutic characteristics of the patients were assessed, with special reference to the INR values on admission (among patients with known AF), and the clinical outcomes. Results - Of the study cohort, 170 patients had a diagnosis of AF before the admission for stroke, but 47% of them did not take anticoagulants. Patients who suffered stroke while on anticoagulants (83 on VKA, 7 on low-molecular-weight heparins), were in most cases (75%) out of the therapeutic INR range, typically undertreated (INR<2). Overall, inadequate or completely absent anticoagulation was documented in 81% of the stroke cases occurring in patients with known AF. Of the entire study cohort, 41% was discharged home, 34% required continued institutional care, and 25% died. Conclusions - The inadequacy or lack of anticoagulation was observed in the vast majority of acute strokes in patients with known AF. These cases are often related to the well-documented limitations of VKA therapy in terms of its safety, tolerability and/or practical aspects. To prevent them, important changes are warranted in the anticoagulation practice, including the closer control of VKA therapy and the broader use of new oral anticoagulants.]
Clinical Neuroscience
JANUARY 30, 2015
[Treatment of osteoporotic vertebral compression fracture with PMMA augmented pedicle screw fixation]
[Background - Over the last few decades many innovative operation technique were developed due to the increase of porotic vertebral fractures. These new techniques aim to reach the required stability of the vertebral column. In case of significant instability, spinal canal stenosis or neural compression, decompressive intervention may be necessary, which results in further weakening of the column of the spine, the minimal invasive percutan vertebroplasty is not an adequate method to reach the required stability, that is why insertion of complementary pedicular screws is needed. Considering the limited screw-fixing ability of the porotic bone structure, with this new technique we are able to reach the appropriate stability of cement-augmented pedicle screws by dosing cement carefully through the screws into the vertebral body. We used this technique in our Institute in case of 12 patients and followed up the required stability and the severity of complications. Methods - Fifteen vertebral compression fractures of 12 patients were treated in our Institute. Using the classification proposed by Genant et al. we found that the severity of the vertebral compression was grade 3 in case of 13, while grade 2 in case of two fractures. The average follow up time of the patients was 22 months (12-39), during this period X-ray, CT and clinical control examinations were taken. During the surgery the involved segments were localised by using X-ray and after the exploration the canulated screws were put through the pedicles of the spine and the vertebral body was filled through the transpedicular screws with bone cement. Depending on the grade of the spinal canal stenosis, we made the decompression, vertebroplasty or corpectomy of the fractured vertebral body, and the replacement of the body. Finally the concerned segments were fixed by titanium rods. Results - In all cases the stenosis of spinal canal was resolved and the bone cement injected into the corpus resulted in adequated stability of the spine. In case of six patients we observed cement extravasation without any clinical signs, and by one patient - as a serious complication - pulmonary embolism. Neurological progression or screw loosening were not detected during the follow up period. Part of the patients had residual disability after the surgery due to their older ages and the problem of their rehabilitation process. Conclusion - After the right consideration of indications, age, general health condition and the chance of successful rehabilitation, the technique appears to be safe for the patients. With the use of this surgical method, the stability of the spine can be improved compared to the preoperative condition, the spinal canal stenosis can be solved and the neural structures can be decompressed. The severity of complications can be reduced by a precise surgical technique and the careful use of the injected cement. The indication of the surgical method needs to be considered in the light of the expected outcome and the rehabilitation.]
Clinical Neuroscience
JANUARY 30, 2015

[Inclusion body myositis]
[The idiopathic inflammatory myopathies are systemic, chronic autoimmune diseases characterized by proximal symmetrical muscle weakness. One of the main diseases in this group is inclusion body myositis (IBM), an underdiagnosed, progressive muscle disease characteristically affecting the middle-aged and older population. It has a slow, relentlessly progressive course. The precise pathogenesis of the disease remains unknown. In most of the cases it is diagnosed a few years after the appearance of the first symptoms. The muscle biopsy typically shows endomysial inflammation, with invasion of mononuclear cells into the non-necrotic fibers, and also rimmed vacuoles. It appers, that both inflammation and degeneration are present at the onset of the disease. Our aim is to raise awareness about this disease which leads to severe disability, with clinicopathological case presentations and literature overview, emphasizing the importance of collaboration between the clinician and the neuropathologist. No effective therapy is currently available but the rapid diagnosis is essential to slow disease progression. Although this is a relatively rare disease, patients are presenting not only in immunology outpatient clinics; our reports aims to raise awareness and facilitate accurate early diagnosis of IBM. ]
Clinical Neuroscience
JANUARY 30, 2015
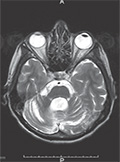
[The first identified Central-Eastern European patient with genetically confirmed dentatorubral-pallidoluysian atrophy]
[Aims - Dentatorubral-pallidoluysian atrophy (DRPLA) is an inherited neurodegenerative disorder characterized by a trinucleotide repeat expansion. The disease mainly occurs amongst the Japanese and is extremely rare in the European population. The characteristic clinical symptoms are cerebellar ataxia, dementia, choreoathetoid movements, epileptic seizures and myoclonus. The aim of this study is to present the first genetically confirmed Hungarian case of DRPLA. Case report - The middle-aged female patient developed the characteristic clinical symptoms except myoclonus over her late thirties with positive family history. The major finding in the skull magnetic resonance imaging was the atrophy of infratentorial brain structures with the consequential dilation of related cerebrospinal fluid spaces. A detailed neuropsychological examination was also performed and it revealed moderate cognitive dysfunctions, mild depression and anxiety. As underlying conditions, Huntington’s disease and common spinocerebellar ataxia forms all came into consideration, but all the result of the respective genetic tests were negative. However, the test for mutation in the ATN1 gene revealed pathological heterozygous CAG repeat expansion. Conclusion - This case study serves as the first description of genetically confirmed DRPLA in the Central-Eastern region of Europe, the clinical features of which seems to be very similar to the previously reported cases.]
Clinical Neuroscience
JANUARY 30, 2015

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.