The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2006;59(07-08)
Content
Clinical Neuroscience
JULY 30, 2006

[THE IMPACT OF MOOD ALTERATIONS ON CREATIVITY]
[Basic elements of artistic (and other) creativity are the technical-professional skill and knowledge, the special talent and ability and the willingness or motivation; one of which being absent results in partially realised creativities like juvenile, frustrated or abandoned types, respectively. Psychometric scales have been developed to measure everyday and eminent creativities, which show that creativity correlates with higher psychoticism, impulsivity and venturesomeness scores and with lower neuroticism and conformity scores of the personality test employed in a general population. Among the psychological components of creativity are the cognitive processes, mood, motivation, and personality traits. Regarding mood, a theory of “inverted U” has been proposed as elevation of mood facilitates creativity to a certain point after what extreme increase has an adverse effect on achievement. Analysing psychopathology and creativity among various professions, higher rates of psychopathology, especially affective symptoms, have been found in art-related professions. Examples of immortal poets, writers, painters, sculptors and composers, having created invaluable cultural treasures for the mankind, illustrate that many of them showed signs of mood alterations (unipolar or bipolar affective disorder spectrum) which were expressed in their artistic products.]



Clinical Neuroscience
JULY 30, 2006
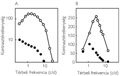
[PARALLEL PROCESSING OF VISUAL INFORMATION]
[This is a survey on the function of parallel visual pathway with a special emphasis on its clinical implications. It is based on data in the literature and own results of our group. The paper primarily deals with the X, Y, W pathways and by the magnocellular, parvocellular and koniocellular visual pathways characterized by cells of various size as well as by nerve fibers of various thickness. Electrophysiological, microelectrode recording of single-unit activity makes the distinction between the pathways available in animal modell. Much more difficulties arise if we intend to characterize the pathways in humans or to detect the selective damage of one of these pathways in patients. The non-invasive diagnostic methods that could be used in the diagnosis are detailed here, too. Finally, the neurological, ophtalmological and psychological diseases are discussed in which a selective damage of any visual pathway is suspected. Summing it up, the survey provides evidences for the introduction of the novel concept of parallel pathways into the diagnostic aspects of ophthalmology, neurology and psychiatry.]
Clinical Neuroscience
JULY 30, 2006

[THE ROLE OF MICRO-AROUSALS IN THE REGULATION OF SLEEP]
[This work give a short account about a three decades research of the sleep microstructure. The studies, executed by the Strassbourg, Budapest and Parma schools, paved the way of exploring the participation of micro-arousals in the sleep regulation. It was shown that micro-arousals, not leading to instant arousal but influencing the later course of sleep are weaved into the network of sleep. A certain class of microarousals differs from the traditional desyncronisation-type and in a paradox way result a rebound like mobilisation of sleeplike activity with deltas and K-complexes. The desynchronisation- and synchronisation-type micro-arousals show different distribution along the sleep cyclicity and may play different role in sleep regulation. On the basis of the studies dealing with micro-arousals we can assume that beside the traditional long time constant, brain stem driven tonic chemical regulation, an other phasic regulation, with shorter time constant, underlied by the micro-arousals, also exist. This kind of phasic regulation makes sleep flexible and possible to adapt the actual sleep course to the inner and outer demands. An other important role of micro-arousals in pathological sleeps is to provide a gate for the different pathological events, pinpointing the key-points where these events could be expected in the sleep process.]
Clinical Neuroscience
JULY 30, 2006
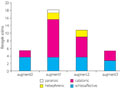
[THE AUGMENTATION OF CLOZAPINE TREATMENT WITH ELECTROCONVULSIVE THERAPY]
[Objectives - The assessment, in terms of safety and efficacy, of augmenting clozapine monotherapy, as well as combined psychopharmacotherapy involving clozapine, with electroconvulsive therapy (ECT). Method - Reviewed were the charts of patients who received clozapine-ECT treatment in the Department of Psychiatry and Psychotherapy of Semmelweis University between November 1999 and December 2003. Results - During the studied period there were altogether 43 patients treated with the combination of clozapine and electroconvulsive therapy. In the schizoaffective group, the values for post-electroconvulsive therapy CGI were significantly lower than either in the catatonic (Z=-3.72, p<0.01) or in the hebephrenic (Z=-3.17, p<0.01) group. Among the groups created on the basis of the number of augmentation strategies utilized, the clozapine+3 group consisted of patients significantly older than the clozapine+1 group (Z=2.45, p=0.01). In the clozapine monotherapy group, the values for post-electroconvulsive therapy CGI were significantly lower than in any of the groups that had received a combination of augmentations (monotherapy-1 augmentation: Z=-3.01, p<0.01; monotherapy-2 augmentation: Z=-2.89, p<0.01; monotherapy- 3 augmentation: Z=-2.41, p=0.01). Conclusions - According to our examinations, the augmentation of clozapine treatment with electroconvulsive therapy should be tried primarily on schizoaffective patients, in case the clozapine monotherapy is ineffective. The simultaneous use of different augmentation strategies is expected to increase only the side effects not the efficacy of the treatment.]
Clinical Neuroscience
JULY 30, 2006

[EXECUTIVE DYSFUNCTION IN FRONTAL LESIONS AND FRONTAL EPILEPSY]
[Background - To explore the functions of the frontal lobe that are associated with high order cognitive and behavioral aspects such as the organization and execution of thoughts and behavior by neuropsychological methods is difficult. These so called executive functions are in close connection with the prefrontal thalamocortical circuits, damage of which can cause deficits in cognitive functions and even changes in personality. Methods - The aim of this study is to present a neuropsychological battery for testing frontal lobe functions. 31 patients (with frontal epilepsy and/or frontal lesion) and 38 healthy control subjects participated in the study. The control subjects were matched to the patient group in age, gender and education. Results - Comparing to the controls the patient group showed significant deficits in most of the measured executive functions, except two tests which show that the short time selective attention is preserved. We divided the patient group into three subgroups (frontal epilepsy only FLE, frontal lesion only FL, frontal lesion and epilepsy FLE+FL) and we found that except working memory deficits and problems in inhibition, there were no difference between the FLE patients and the control group. We found most frequently perseveration and errors in a strategy making task among the FL (mainly medial) patients. We didn’t find any difference in these tests according to the lateralization of the lesion. Conclusion - In conclusion we found that working memory deficits and problems in inhibition differentiated the frontal patient group from the controls in all cases. We emphasize that in frontal epilepsy (with no reported MR lesion) there are the same type, however more limited neuropsychological alterations as in lesional frontal dysfunction.]
Clinical Neuroscience
JULY 30, 2006
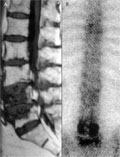
[APPLICATION OF VERTEBROPLASTY, NEURONAVIGATION AND KYPHOPLASTY IN THE TREATMENT OF MULTIPLEX OSTEOPOROTIC VERTEBRAL FRACTURES - CASE REPORT]
[Vertebroplasty is a therapeutic image-guided procedure, consisting of an injection of acrylic cement through a bone biopsy needle into a vertebral body. Main indication for vertebroplasty is painful vertebral body compression fracture due to osteoporosis. The procedure is an efficient mean with high succes in pain release and prevention of further collapse of the treated vertebrae; however, the technique does not allow to realign the spine. Kyphoplasty was designed to adress the kyphotic deformitiy. It involves the percutaneous placement of an inflatable bone tamp into a vertebral body (VB). Restoration of VB height and kyphosis correction is achieved by inflation of the tamp with contrast material liquid. After deflation a cavitiy is created that eases the cement application. The most modern way of guidance in spinal surgery is neuronavigation - the use of frameless stereotaxy. The system reformats patient-specific CT images acquired prior surgery, performs image fusion with intraoperative plain X-ray. Before the operation, the surgeon may create surgical plan and simulate advancement of a virtual instrument along one or more surgical trajectories. During surgery, the system tracks the position of specialized surgical instruments. All three modalities mentioned above have been applied in the treatment of our patient suffered from multiple osteoporotic vertebral body compression fractures. Using kyphoplasty an almost total VB height restoration could be achieved. The pain relief was more than 50% after both operation.]
Clinical Neuroscience
JULY 30, 2006

[AIDS-RELATED TOXOPLASMA-ENCEPHALITIS PRESENTING WITH ACUTE PSYCHOTIC EPISODE]
[The most frequent neurological manifestations of the Acquired Immunodeficiency Syndrome- (AIDS) are Cerebral Toxoplasmosis, Primary Central Nervous System Lymphoma (PCNSL), Progressive Multifocal Leukoencephalopathy (PML) and AIDS-encephalitis (AIDS-dementia complex, multinucleated giant cell encephalitis, HIV-encephalopathy). Neurological complications usually occur in the advanced stages of the disease, and they are uncommon in the beginning as presenting illness, but may result in lifethreatening condition or in death. Rarely the disease presents as a neuropsychiatric illness in an undiagnosed AIDS patient, delaying a proper diagnosis. We present the case of a 34 years old patient treated for AIDS-related Toxoplasma-encephalitis in our department. His illness started as an acute psychosis followed by rapid mental and somatic decline, leading to death in three months. His HIV-seropositivity was not known at his admission, and the extraneural manifestations were slight. The diagnosis was established by serology, imaging methods and histopathological investigation. After presenting the medical history and results of autopsy studies of the patient we discuss the problems of the differential diagnosis, especially regarding the findings of the imaging methods.]
Clinical Neuroscience
JULY 30, 2006

Clinical Neuroscience
JULY 30, 2006

Clinical Neuroscience
JULY 30, 2006

[Account on the Senate of the Hungarian Society of Neurology and Psychiatry]
[Account on the Senate of the Hungarian Society of Neurology and Psychiatry 2006;59(07-08)]
1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.