The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2006;59(03-04)
Content
Clinical Neuroscience
MARCH 30, 2006

[CURRENT ISSUES IN NEUROUROLOGY]
[The author gives an overview on the pathophysiology and management of neurogenic bladder dysfunction and lists the most common bladder dysfunctions observed in various diseases of the nervous system. The cited classifications, principles, and categories follow the current guidelines of WHO and the International Continence Society. The author and his co-workers have been involved in the rehabilitational treatment of patients with neurogenic bladder dysfunction for more than a decade. The review paper is supplemented with illustrations taken from the author's own cases.]



Clinical Neuroscience
MARCH 30, 2006

[PLASTICITY OF NOCICEPTION: RECENT ADVANCES IN FUNCTION-ORIENTED STRUCTURAL PAIN RESEARCH]
[Traditional concept holds that the pain unit consists of three neurons. The first of these, the primary nociceptive neuron, starts with the nociceptors and terminates in the dorsal spinal cord. The second one, called spinothalamic neuron, crosses over in front of the central canal and connects the dorsal horn with the thalamus. The third one, called thalamo- cortical neuron, terminates in the “pain centres” of the cerebral cortex. While this simplistic scheme is useful for didactic purposes, the actual situation is more complex. First, in the periphery it is only nociception that occurs, while pain is restricted to the levels of thalamus and the cortex. Second, pain results from interactions of excitation and inhibition, from divergence and convergence and from attention and distraction, in a diffuse and plastic system, characteristic for all levels of organization. This study describes the major cytochemical markers of primary nociceptive neurons followed by the presentation of recent data on the functional anatomy of nociception and pain, with special focus on the intrinsic antinociceptive system and the role of nitrogen oxide, opiate receptors, nociceptin and nocistatin. In addition to the classic intrinsic antinociceptive centres such as the periaqueductal gray matter and the raphe nuclei, roles of several recently discovered members of the antinociceptive system are discussed, such as the pretectal nucleus, the reticular formation, the nucleus accumbens, the nucleus tractus solitarii, the amygdala and the reticular thalamic nucleus, this latter being a coincidence detector and a centre for attention and distraction. The localisation of cortical centres involved in the generation of pain are presented based on the results of studies using imaging techniques, and the structural basis of corticospinal modulation is also outlined. Seven levels of nociception and pain are highlighted where pharmacological intervention may be successful, 1. the peripheral nociceptor, 2. the spinal ganglion, 3. the multisynaptic system of the dorsal horn, 4. the modulatory system of the brain stem, 5. the antinociceptive system, 6. the multisynaptic system of the thalamus, and 7. the cortical evaluating and localisation system that is also responsible for descending (inhibiting) control. The many levels of nociception and pain opens new ways both for pharmacological research and the general practitioner aiming to alleviate pain.]
Clinical Neuroscience
MARCH 30, 2006

[THE USE OF INTRAVENOUS IMMUNGLOBULIN IN THE TREATMENT OF AUTOIMMUNE NEUROMUSCULAR DISEASES]
[Intravenous immunglobulin given in autoimmune neuromuscular disorders modulates the immune system by complex actions, including, 1. the modification of the expression and function of Fc receptors, 2. interference with the activation of the complement and the cytokine network, 3. neutralisation of antiidiotypic antibodies, 4. effects on the activation, differentiation and effector functions of the T and B cells. Controlled trials have shown that intravenous immunglobulin is effective as first-line therapy in patients with Guillain-Barré syndrome and multifocal motor neuropathy. In case of steroid resistance or coexisting diabetes mellitus, intravenous immunglobulin can be the first line therapy in chronic inflammatory demyelinating polyneuropathy as well. As an alternative therapy it can be a second-line choice in dermatomyositis, myasthenia gravis, Lambert-Eaton myasthenic syndrome, and stiff person syndrome. While it has a remarkably good safety record for long term administration the following side effects have been observed: headache, skin rash, thromboembolic events and renal tubular necrosis. In some disorders, the appropriate dose and frequency of infusions that maintain a satisfactory therapeutic response is well defined on the basis of data of evidencebased medicine, whereas in others it still remains to be defined. For the analysis of pharmacoeconomical aspects and the mechanism(s) of response differences in the same disease categories, further studies are necessary.]
Clinical Neuroscience
MARCH 30, 2006
[INTERACTIONS BETWEEN THE MTHFR C677T AND MTHFR A1298C MUTATIONS IN ISCHAEMIC STROKE]
[Introduction - Methylenetetrahydrofolate reductase (MTHFR) C677T and A1298C mutations, being considered unfavourable genetic factors by causing elevated serum homocysteine levels, may be risk factors for cardiovascular disorders, including ischaemic stroke. In this study, the role of these two mutations in ischaemic stroke was examined. Patients and methods - Genetic and clinical data were analysed of 122 ischaemic stroke patients and 102 control subjects with no lesions by neuroimaging. Results - Neither of the two MTHFR mutations alone was found to be a significant genetic risk factor for ischaemic stroke. However, at least one MTHFR 677T allele combined with at least one MTHFR 1298C allele significantly increased the risk of ischaemic stroke (adjusted odds ratio: 3.39; p<0.001). Conclusion - The synergistic effect between the two MTHFR mutations may represent a new genetic stoke risk factor.]
Clinical Neuroscience
MARCH 30, 2006

[ULTRASONOGRAPHIC EXPRESSIONS OF THE FOETAL FACE MAY REFLECT FOETAL MOOD - MIMICRY IS PART OF FOETAL ETHOLOGY]
[The author studied foetal faces and changes in features in the coronal plane during routine prenatal ultrasound scans. Based on known behaviour of children and adults, deductions can be made about foetal mood alterations. During the four years of the study the author noted five main facial expression changes that might be reflections of foetal mood. Foetal expressions and fine lineaments may indicate adequate maturity of the central nervous system as well as satisfactory oxygen supply. Ethologically, facial mimicry is an inherited behavioural pattern.]
Clinical Neuroscience
MARCH 30, 2006
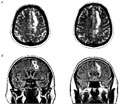
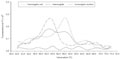
[SPECTRAL EEG-CHARACTERISTICS OF SUBCORTICAL ISCHEMIC BRAIN LESION- A CASE STUDY]
[Introduction - Although the EEG-changes caused by ischemic stroke are well known, data of the literature are rather ambiguous. The EEGfindings recorded in a patient with a unilateral subcortical ischemic lesion are evaluated with special emphasis related to the effect of the dynamics caused by eyes opening. Participants and methods - Data recorded from a patient (54 years old male with a completed stroke involving the frontal and parietal subcortical region in the left side) were compared to those of a control group (12 healthy age matched subjects). Absolute and relative frequency spectra, theta/beta quotients, the interaction index characterizing the effect of eyes opening and the symmetry index were calculated from the EEG recorded in eyes closed and eyes open conditions. Data of the patient were compared to those recorded in the control group on the basis of 95% confidance intervals. Results - Irrespective of the recording conditions the predominance of slow activity and the increase of theta/beta quotients were found in the absolute frequency spectra. The increase of beta1 and beta2 frequency bands following eyes opening on the side of the lesion were found to be less obvious than that seen on the intact side and that observed in the control group. With respect to the interaction index related to the side differences caused by eyes opening the change of the beta2 frequency band was found to be the most conspicuous. The symmetry index underscored the predominance of slow (delta, theta, alpha1) frequencies on the lesion side, and that of the fast (beta1, beta2) frequencies on the intact side in both recording conditions. Conclusions - Localized lesion of the white matter without cortical damage can cause the predominance of slow activity and decrease of the fast frequency bands on the side of the lesion which can be shown by the absolute frequency spectra and is revealed by the symmetry index. The lack of functional reactivity of the fast frequencies in the side of the lesion can clearly be seen in the change of relative spectra following eyes opening and on the basis of the calculation of the interaction index reflecting the dynamics of side differences.]
Clinical Neuroscience
MARCH 30, 2006

[Drug problems, psychopathology in youth, sociocultural background factors]
[Drug problems, psychopathology in youth, sociocultural background factors 2006;59(03-04)]
Clinical Neuroscience
MARCH 30, 2006

Clinical Neuroscience
MARCH 30, 2006

Clinical Neuroscience
MARCH 30, 2006

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
3.
4.
5.