The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Clinical Neuroscience - 2005;58(05-06)
Content
Clinical Neuroscience
MAY 10, 2005

[Pathophysiology of restless leg syndrome and periodic leg movement disorder in view of the latest research findings]
[Both restless leg syndrome and periodic leg movement disorder have been classified as primary sleep disorders by the International Classification of Sleep Disorders. Considering the characteristic clinical symptoms, it is supposed that their pathomechanism involves the peripheral and central stimulusprocessing mechanisms of the nervous system as well as several elements of the motor system. During the last couple of years many new elements of the pathomechanism have been discovered, in particular the dysfunction of the postsynaptic dopamin receptors related to the iron metabolism of the central nervous system, the role of opiate receptors, and the involvement of subclinical small fiber neuropathy. Many of these findings have been incorporated into the diagnostic and treatment protocols used in the management of patients with restless leg syndrome or periodic leg movement disorder. Considering the rapidly increasing number of publications on their pathomechanism and the various fields it involves, the authors found it necessary to evaluate these data and to interpret their relationships within the frame of sleep-wake regulation.]



Clinical Neuroscience
MAY 10, 2005

[Frontotemporal dementia - Part I History, prevalence, clinical forms]
[The authors report a comprehensive publication consisting of three parts going into the details of history, prevalence, clinical forms, differential diagnosis, genetics, molecular pathomechanism, pathology, clinical diagnosis and treatment of frontotemporal dementia (FTD). The first part of the present review deals with history, prevalence and clinical forms of FTD. The prototypical FTD with circumscribed atrophy was first described by Arnold Pick; Alois Alzheimer found the intraneural inclusions in the patients’ brain. Later it was recognised that many patients had neither the atrophy nor the cellular changes, but genetic mutations have been identified. Frontotemporal dementia is a degenerative condition with unknown etiology in the frontal and anterior temporal lobes of the brain. It is a progressive neurobehavioral syndrome characterized by early decline in social interpersonal conduct, early impairment in the regulation of personal conduct, early emotional blunting, and early loss of insight. There are no reliable epidemiological studies on the prevalence of FTD, but it is well-accepted that FTD is a common cause for dementia before the age of 65 (it constitues approximately five percent of all irreversible dementias). The nomenclature of the FTD has been confusing and continues to be. Three major clinical syndromes can be identified: 1 frontal variant FTD (dementia of frontal type) in which changes in social behavior and personality predominate, 2. in semantic dementia (progressive fluent aphasia) there is a breakdown in the conceptual database which underlies language production and comprehension, 3. in progressive nonfluent aphasia the phonologic and syntactic components of language are affected. The authors report two cases, which can point to clinical symptoms and forms, and mention the problems of the differential diagnosis and therapy.]
Clinical Neuroscience
MAY 10, 2005

[THE SELECTIVE COX-2 INHIBITOR MELOXICAM AND SALICYLATE THERAPY]
[Although during treatment of arthrosis with meloxicam the level of thromboxan A2 decreases, thrombocyte functions are not affected. Meloxicam in therapeutic doses doesn’t increase the risk of haemorrhage. Previously it was suspected that coadministration of salicylates with certain other non-steroid antiinflammatory drugs (NSAIDs) will suppress the effect of salicylate. Van Ryn et al have proved that this is not the case with salicylate plus meloxicam therapy. It is hypothesized that meloxicam loosely binds to the cyclooxygenase-1 (COX-1) enzyme and salicylate can easily replace it.]
Clinical Neuroscience
MAY 10, 2005

Clinical Neuroscience
MAY 10, 2005
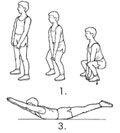
[Primary prevention program of the Hungarian Spine Society - Part II Controlled prospective study of short term efficacy]
[Introduction - The primary prevention program of the Hungarian Spine Society is set around 12 test exercises that assess performance of postural muscles and then develops their strength and flexibility. By this the scheme aims to make the biomechanically correct use of the spinal column spontaneous. Subjects and methos - The application of the scheme in the frame of physical education in a primary school was investigated in a prospective controlled study in the school-year of 2001/2002. Participating children were aged 6 to 14. The intervention group (n=200) regularly did the posture correction exercises with their teacher's direction in physical education classes, while the control group (n=213) did not. The 12 test exercises of the posture correction scheme of the Hungarian Spine Society were tested by an independent physiotherapist at the beginning and at the end of the school-year in both groups. Results were analyzed by paired and unpaired t-tests and by a chi-square test. Results - At the end of the school-year the strength and flexibility of the postural muscles of the intervention group improved significantly compared both to their own performance (p<0.01) at the beginning of the school-year and to the control group. Test results of the control group were significantly (p<0.05) worse at the end of the school-year than their own results at beginning of the school-year, and were more significantly (p<0.01) worse than the test results of intervention group. Conclusion - The results of the controlled study confirm that regular use of the preventive exercises in physical education improves the strength and flexibility of postural muscles. In order to analyze the results concerning specific muscle groups or age groups a detailed study with age- and gender-matched controls will be necessary.]
Clinical Neuroscience
MAY 10, 2005
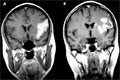
[A case history and diagnostical rewiev of primary cerebral angiitis]
[The authors present a case history of primary cerebral angiitis with four years of follow-up. The early diagnosis was based on typical clinical symptoms, brain MRI, intracerebral MRA and histology of sural nerve biopsy. Electroneurography suggested peripheral involvement, although the patient did not have clinical signs of peripheral neuropathy. Glucocorticoid and immunosuppressive treatment resulted in remission. The diagnostic difficulties of primary cerebral vasculitis are also summarized in the discussion.]
Clinical Neuroscience
MAY 10, 2005

Clinical Neuroscience
MAY 10, 2005
Clinical Neuroscience
MAY 10, 2005

Clinical Neuroscience
MAY 10, 2005

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
3.
4.
5.