The eLitMed.hu medical portal uses computer cookies for convenient operation. Detailed information can be found in the Cookie-policy.
Lege Artis Medicinae - 2004;14(04)
Content
Lege Artis Medicinae
APRIL 21, 2004




Lege Artis Medicinae
APRIL 21, 2004

[ANTICOAGULATION AND THROMBOEMBOLIC DISEASES - INDICATIONS, PROBLEMS AND PRACTICAL ASPECTS]
[The widespread application of the LMW heparins promoted the prevention and therapy of the thromboembolic diseases in Hungary. Their propagation is mainly due to their simple clinical application and the active promotion of the producing pharmaceutical companies. However, the recommended “unnecessary” (in the reality the lack of) laboratory control may cause severe complications (bleeding, thromboembolism etc.) sometimes especially at the therapeutic application. For this reason, unfractionated (UF) heparin is advised in case of acute deep vein thrombosis when a patient is in the particular danger of bleeding because of its better controllability and the opportunity to stop anticoagulation immediately. In recent years, the indication of the long-term anticoagulation therapy expanded significantly. The number of patients is ever growing who need continuous anticoagulation because of atrial fibrillation or venous thromboembolic episode taken place earlier. Large randomised multicenter trials proved the efficacy of prolonged coumarin therapy in the prevention of recurrence of thromboembolic episodes in these diseases. Due to its advantageous pharmacological characteristics warfarin is especially suitable for the attainment of continuous anticoagulation. The direct thrombin inhibitor melagatran (and its orally applicable form, ximelagatran) may open a new era in the prophylaxis and therapy of the thromboembolic diseases. Its advantageous pharmacological characteristics and its simple application may make them to the antithrombotics of the future in case of a reasonable price and/or subsidisation.]
Lege Artis Medicinae
APRIL 21, 2004

Lege Artis Medicinae
APRIL 21, 2004
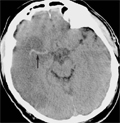
[THE IMPORTANCE OF HYPERTENSION IN CEREBROVASCULAR DISEASES]
[Stroke is a highly prevalent disorder worldwide; it is the third main cause of death and the leading cause of severe disability. Recent data showed that 72-86% of cerebrovascular disorders are of ischaemic type. Arterial hypertension is the most prevalent risk factor for both haemorrhagic and ischaemic stroke, it is present in approximately 70% of cases. All forms of hypertension, isolated systolic or diastolic and combined hypertension increase stroke risk about 3-4 times and the relationship with systolic blood pressure may even be stronger than with diastolic blood pressure. Hypertension is very common after acute stroke. In this phase the cerebral autoregulation is disturbed in the region of focal brain ischaemia or haemorrhage such that cerebral blood flow is directly dependent on systemic blood pressure. It is therefore essential to avoid systemic hypotension in acute stroke patients and the reduction of high blood pressure may lower cerebral blood flow in the ischemic penumbra. Evidence from clinical data shows that control of blood pressure leads to lower risk of first or reccurent stroke and patients have shown beneficial effects especially of ACE inhibitors and diuretics. In the PROGRESS study both hypertensive and non-hypertensive cerebrovascular patients benefited from antihypertensive therapy. Previous results suggests that there may be additional beneficial effects of the ACEinhibitor therapy not related to blood pressure lowering in the prevention of stroke.]
Lege Artis Medicinae
APRIL 21, 2004

[HUMAN DENDRITIC CELLS AND INFECTIVE AGENTS]
[Dendritic cells represent important components of the innate and adaptive immune responses. Human dendritic cells can be divided into two major subsets: myeloid and plasmacytoid (lymphoid) dendritic cells. The unique function of the dendritic cells is to capture antigens, present and to activate the antigenic peptides to the T lymphocytes. Dendritic cells go through a maturation process both in vitro and in vivo. By the use of pathogenrecognition- receptors the immature dendritic cells sense diverse pathogens or their various components, or cellular factors produced by the infected neighboring non-dendritic cells, and maturation signals are transduced for the dendritic cells. The heterogeneity of the pathogen-recognition-receptors and the microbial stimuli initiate a broad range of interactions between dendritic cells and infectious agents. Dendritic cells infected with certain viruses produce only a few infectious particles, but express and present viral antigens to T lymphocytes and immune response is initiated (influenza virus). Dendritic cells infected with certain pathogens not only initiate immune response but also disseminate the pathogen (human immunodeficiency virus, Mycobacterium tuberculosis). Some pathogens are killed in the dendritic cells, but the antigens are presented to the T cells, and immune responses are induced (Chlamydia trachomatis and Chlamydia psittaci). Dendritic cells capture antigens produced by infected neighbouring cells and present them to T lymphocytes, thus immune response is initiated (human cyto-megalovirus, herpes simplex virus). Dendritic cells are responsible for virus-induced immunosupp-ression; dendritic cells infected with certain pathogens form syncytia with T cells, thereby contribute to the suppression of T cell functions directed against opportunistic infections (measles virus). Dendritic cells can present not only foreign antigens but also self-antigens and when immature dendritic cells become mature upon exposure to inflammatory processes or to pathogens capable of activating them they can induce autoimmunity.]
Lege Artis Medicinae
APRIL 21, 2004
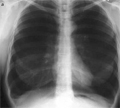
[THE PROSPECTS OF SURGICAL TREATMENT OF END-STAGE EMPHYSEMA (COPD): THE LUNG VOLUME REDUCTION SURGERY]
[On the basis of relevant international literature the author presents the indications, contraindications, risks and results of the lung volume reduction surgery applicable in cases of therapyresistant end-stage COPD. These interventions, which require strong interdisciplinary cooperation of a pneumonologist, a thoracic surgeon, an anaesthesiologist and a physiotherapeutist were introduced in 1995 as a result of Cooper's study. A multicentric prospective study analysed the efficiency of this new surgical procedure. The results were evaluated in 2003 and it is important to be emphasised that in short term (3-6 months) and medium term (2-4 years) an improvement of lung function and of the quality of life can be observed in those patients who have heterogeneous emphysema, mainly in the upper lobe. Also, in case of homogenous emphysema this surgical procedure can be effective but perioperative mortality is higher and a deterioration in the health-state can occur as soon as six month after the intervention. The follow-up analyses of COPD patients with alpha- 1 antitrypsin deficiency show similarly moderate results. In Szombathely, Hungary 67 such interventions were carried out on 55 patients between 1997 and 2002, with a 4.4 % mortality rate which corresponds the international standard. Our own experience also supports the fact that in short and medium term the FEV1, RV, paO2, paCO2 and the quality of life take a positive change, the continuous O2-demand of patients will cease to exist and they regain parts of the former activity. The LVRS bears remarkable cost due to the use of staplers and surgical materials as well as longer hospital stay with the need of intensive care unit. Today in Hungary the LVRS is a realistic alternative in case of severe COPD to lung transplantation. The cost of an LVRS is maximum 10% of a lung transplantation. Patients having undergone an LVRS as well as patients unacceptable for LVRS may be suitable for lung transplantation.]
Lege Artis Medicinae
APRIL 21, 2004

Lege Artis Medicinae
APRIL 21, 2004

Lege Artis Medicinae
APRIL 21, 2004

1.
Clinical Neuroscience
[Headache registry in Szeged: Experiences regarding to migraine patients]
21. MAY
2.
Clinical Neuroscience
[The new target population of stroke awareness campaign: Kindergarten students ]
21. MAY
3.
Clinical Neuroscience
Is there any difference in mortality rates of atrial fibrillation detected before or after ischemic stroke?
27. NOV
4.
Clinical Neuroscience
Factors influencing the level of stigma in Parkinson’s disease in western Turkey
27. SEP
5.
Clinical Neuroscience
[The effects of demographic and clinical factors on the severity of poststroke aphasia]
18. JUL
1.
2.
Clinical Oncology
[Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up]
29. AUG
3.
Clinical Oncology
[Pharmacovigilance landscape – Lessons from the past and opportunities for future]
29. AUG
4.
5.